


Abstract
Background: Despite several clinical trials and advances in understanding the genetic basis of biliary tract cancer (BTC), the addition of epidermal growth factor receptor (EGFR) targeted therapy does not seem to enhance the activity of first-line chemotherapy (CHT). Materials and Methods: We carried out a meta-analysis of available randomized clinical trials to assess the efficacy and safety of gemcitabine-based first-line CHT plus monoclonal antibodies against EGFR (EGFR-mAbs) in advanced or metastatic BTC. Results: In the overall population, the pooled hazard ratio for overall (OS) and progression-free (PFS) survival were 0.82 (95% confidence interval=0.64-1.06) and 0.88 (95% confidence intervaI=0.73-1.08), respectively. No differences were detected in objective response rate between the two groups. Patients treated with gemcitabine-based CHT plus EGFR-mAbs showed a statistically significant increased risk of grade 3-4 neutropenia, grade 3-4 thrombocytopenia and especially grade 3-4 skin rash. Conclusion: The addition of EGFR-mAbs to gemcitabine-based first-line CHT does not significantly improve overall and progression-free survival, nor the objective response rate in patients with advanced BTC and increases the risk of hematological and cutaneous adverse drug events.
Biliary tract cancer (BTC) is the second most common primary liver tumor accounting for approximately 10-15% of all hepatobiliary malignancies and 3% of all gastrointestinal neoplasms (1-3). BTCs include a heterogeneous group of malignancies usually divided into intrahepatic cholangiocarcinoma (iCCA), extrahepatic cholangiocarcinoma (eCCA), gallbladder cancer (GBC) and ampulla of Vater cancer (AVC), according to anatomical location (4, 5). Although traditionally considered rare tumors in Western countries, their incidence and mortality rate are on the whole rising worldwide. In particular, the incidence of iCCA is expected to further increase in the near future (6-9). Currently, radical surgery with microscopically negative resection margins is the only potentially curative therapy available, although most patients are diagnosed in late disease stages (locally advanced/unresectable or metastatic) (10, 11). Moreover, even after complete surgical resection, the recurrence rate is high and the 5-year overall survival (OS) rate remains discouraging (20-35% at 5 years) (12-14). Cisplatin plus gemcitabine is currently considered the standard first-line treatment for advanced or metastatic BTC, based on the results of the ABC-02 trial, where the OS was 11.7 months compared to 8.1 months in the gemcitabine single-agent arm [hazard ratio (HR)=0.64, 95% confidence intervaI (CI)=0.52-0.80; p<0.001] (15). The combination of gemcitabine and oxaliplatin is widely used in clinical practice in light of a similar antitumoral activity and a favorable safety profile compared to cisplatin – gemcitabine combination (16-18). Nevertheless, the prognosis of advanced or metastatic BTC is still poor, with an OS generally lower than 12 months (19, 20).
As a result of the increasing availability of genomic sequencing data, many signaling pathways and new genetic aberrations involved in the carcinogenesis of BTC have recently been delineated (21).
The mitogen-activated protein kinase (MAPK) pathway consists of a series of low-molecular-weight GTP-binding proteins related to the transduction of signals from cell surface receptors to the nuclear DNA (22). RAS represents the first step of this pathway and is involved in several biological processes including proliferation, growth, senescence and survival (23, 24). KRAS mutations and epidermal growth factor receptor (EGFR) overexpression are reported as common genetic alterations in BTC, whose frequency varies in the different anatomical subtypes (25-28). In a study by the Mayo Clinic group, KRAS mutations were detected in six out of 67 (9%) cases of iCCA (29); in a Japanese study, these mutations were found in 10 out of 22 cases of iCCA (45%), in 24 out of 36 cases of eCCA (67%) and in 16 out of 19 GBC (84%) (30). KRAS mutation has been associated with aggressive disease, reduced survival and perineural invasion in every anatomical subtype of BTC (31).
Several clinical trials have recently evaluated the role of EGFR-targeted drugs, usually divided into EGFR tyrosine kinase inhibitors (EGFR-TKIs) and monoclonal antibodies to EGFR (EGFR-mAbs), with disappointing results as monotherapy or in combination with chemotherapy (CHT) (32-37). Anti-EGFR agents are widely used in head and neck cancer, lung and colorectal cancer, given the benefits provided by these targeted therapies in the advanced or metastatic setting (38-41).
The aim of our meta-analysis was to evaluate the efficacy [in terms of OS, progression-free survival (PFS) and objective response rate (ORR)] and safety of gemcitabine-based CHT plus EGFR-mAbs in patients with advanced or metastatic BTC.
Materials and Methods
Search strategies. All phase II and III randomized clinical trials published until November 2, 2019 which compared gemcitabine-based first-line CHT plus EGFR-mAbs versus gemcitabine-based first-line CHT alone were selected (by A.R. and G.F.). Key words used for searching on PubMed/Medline, Cochrane library, and EMBASE were: “Gemcitabine”, “EGFR-TKIs”, “EGFR-mAbs”, “EGFR”, “Target Therapy”, “Biliary Tract Cancer”, “Cholangiocarcinoma”, “Randomized Controlled Clinical Trial” and “Clinical Trial”. Only articles published in peer-reviewed journals and written in the English language were considered. Furthermore, proceedings of the main international oncological meetings (American Society of Clinical Oncology, European Society of Medical Oncology, European Council of Clinical Oncology, American Association for Cancer Research, European Association of Gastroenterology, and Asian Pacific Association of Gastroenterology), were also searched from 2005 onward for relevant abstracts. Studies selected from the first analysis were then restricted to clinical trials and reviewed (by A.R. and G.F.). This meta-analysis was conducted according to Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines.
Types of outcome measures. Outcomes were divided into two groups: efficacy and toxicity. Efficacy outcomes included OS, PFS and ORR. OS was defined as the time from the date of random assignment to date of death as a result of any cause; PFS was defined as the time from random assignment in a clinical trial to disease progression or death from any cause. ORR included complete response and partial response. Toxicity data were classified according to World Health Organization (WHO) or National Cancer Institute Common Toxicity Criteria (NCI-CTC) (42). We analyzed the most frequently reported grade 3-4 adverse events (ADEs).
Data extraction and synthesis. The following data were extracted for each publication: a: Study general information (author, year, phase, carry out country); b: primary site (iCCA, eCCA, GBC, AVC); c: interventions; d: dosage of drugs; e: number of patients; f: OS and PFS expressed as HRs for patients treated with combination therapy versus gemcitabine-based CHT alone; g: ORR; h: side-effects. Two separate Authors (A.R. and G.F.) conducted the search and identification independently.
Statistical design. Co-primary endpoints of the meta-analysis were OS and PFS for all patients. Meta-analyses were performed using Review Manager (Rev-Man 5.3) software, Version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). Time-to-event data (OS, PFS) were expressed as HRs of combination therapy over gemcitabine-based CHT alone, with 95% confidence intervals (CIs). The inverse variance technique was applied for the meta-analysis of the HR. Relative risks (RRs) were used to analyze dichotomous variables, including ORR and grade 3-4 adverse events; RRs were combined with Mantel–Haenszel method. Statistical heterogeneity between studies was examined using the chi-square test and the I2 statistic. Substantial heterogeneity was considered to exist when the I2 value was greater than 50% or there was a low p-value (<0.10) from the chi-square test.
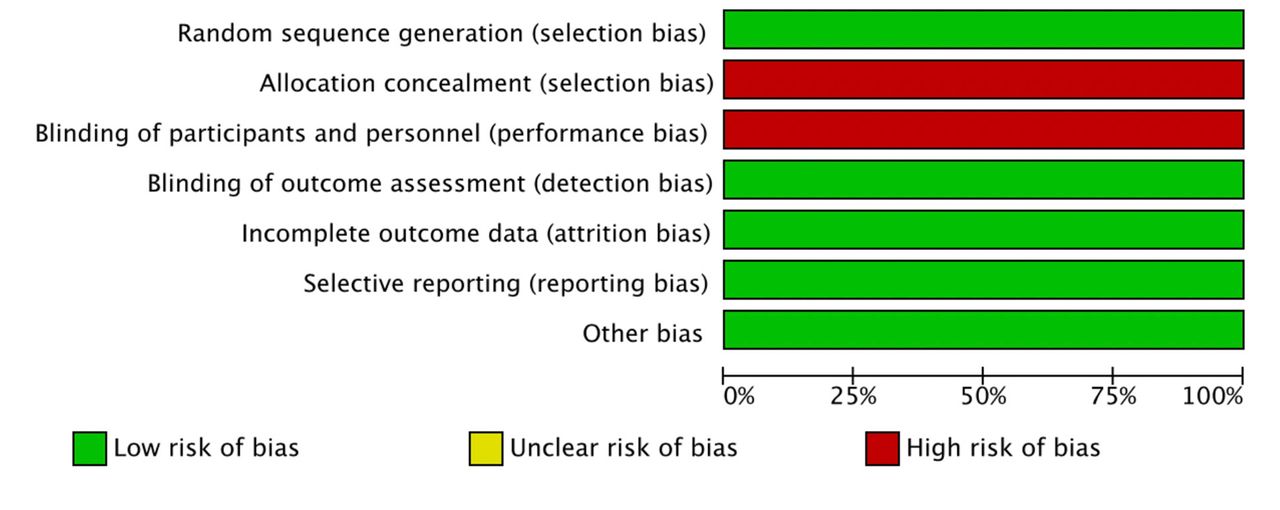
Assessment of risk of bias in included studies. Two authors (A.R and G.F.) independently assessed the risk of bias in included studies using the tools of The Cochrane Collaboration for assessing risk of bias (43): selection, performance, detection, attrition and reporting bias. Reporting bias was assessed by comparing the lists of outcomes from study protocols or trials registries to those reported in the published paper. The results were summarized in both a risk of bias graph (Figure 1) and a risk of bias summary (Figure 2). We interpreted the results of the meta-analyses in the light of the findings according to risk of bias.
Results
Studies selected. The search of electronic databases provided a total of 1,459 citations. An additional 45 records were identified from conference proceedings and trial registries, making a total of 1,504 search results. After adjusting for duplicates, excluding irrelevant topics, 24 records remained for examination in more detail. Eleven were excluded as there were no control arms and four were ongoing trials. Five randomized clinical trials (RCTs) were excluded because the experimental arm consisted of EGFR-TKIs. This left four RCTs to be included after independent evaluation of two Authors (A.R. and G.F.) (33-36). Figure 3 shows the search process.
A total of four RCTs comparing gemcitabine-based CHT plus EGFR-mAbs with gemcitabine-based CHT as first-line treatment were selected, including a total of 450 patients (228 in the combination arm, 222 in the gemcitabine-based CHT alone arm) (33-36). Both published full articles and study protocols were available in all four studies. One study was conducted in Italy (34), one in Taiwan (33), one in Germany (36) and one in France and Germany (35). All of the studies provided complete data for OS analysis, for PFS analysis and for grade 3-4 toxicities; three studies provided complete data for ORR. A summary of the included RCTs is presented in Table I.
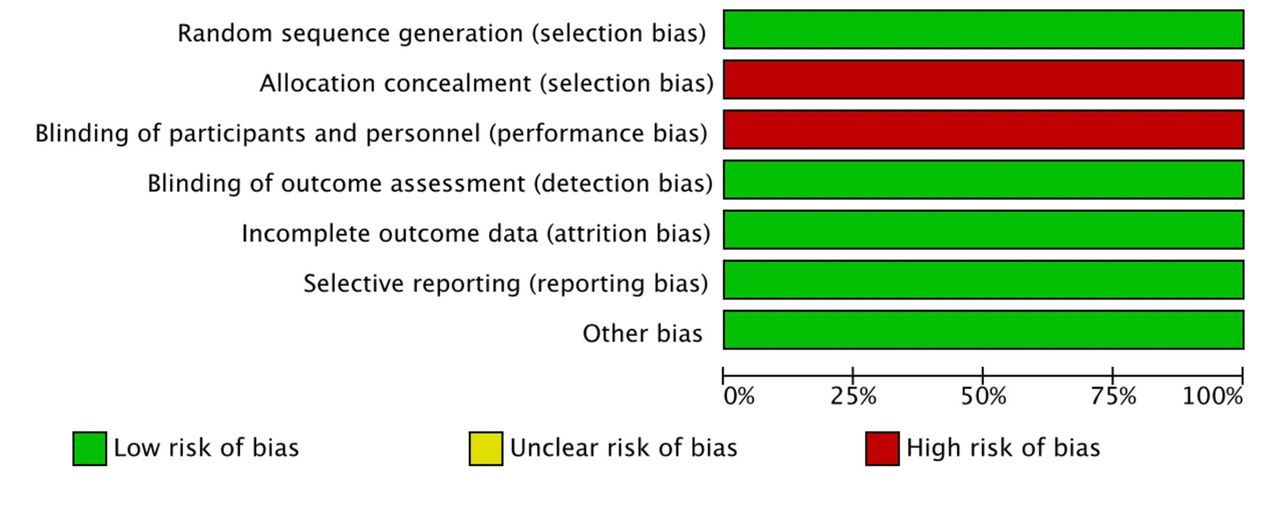
Risk of bias graph: Authors' judgements on each risk of bias item presented as percentages across all included studies.
OS. Four studies provided OS data on 450 patients affected by advanced BTC (33-36). The median OS ranged from 9.9 to 12.8 months in the combination of gemcitabine-based CHT with EGFR-mAbs and was 9.8-20.8 months for CHT alone. Addition of EGFR-mAbs did not show a significant OS benefit (pooled HR=0.82, 95% CI=0.64-1.06) (Figure 4); the analysis was associated with a moderate level of heterogeneity (I2 value of 33%). Results did not differ whether fixed or randomized model effects were adopted.
PFS. The median PFS ranged from 5.3 to 6.7 months in the gemcitabine-based CHT plus anti-EGFR-mAbs arm and was 4.1-8.3 months for CHT alone; the addition of EGFR-mAbs to CHT did not result in a significant PFS benefit when compared to gemcitabine-based CHT alone (pooled HR=0.88, 95% CI=0.73-1.08) (Figure 5).
ORR. Three studies provided objective response rate data on 361 patients affected by advanced BTC (33-35). No ORR superiority was reported by the addition of EGFR-mAbs, with a pooled RR of 1.34 (95% CI=0.91-1.99) (Figure 6).
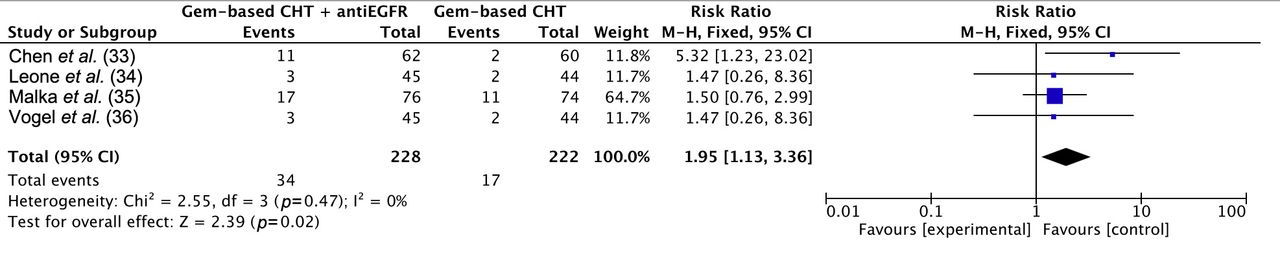
Toxicity. We assessed five types of frequently occurring grade 3-4 ADEs in terms of neutropenia, thrombocytopenia, skin rash, diarrhea and fatigue during the current analysis (Figures 7, 8, 9, 10 and 11). Patients treated with gemcitabine-based first-line CHT and EGFR-targeted therapy had higher risk of neutropenia (RR=1.95, 95% CI=1.13-3.36), thrombocytopenia (RR=1.69, 95% CI=0.99-2.87) and especially skin rash (RR=18.11, 95% CI=5.13-63.91). In addition, we compared the incidence of diarrhea (RR=2.01, 95% CI=0.91-4.44) and fatigue (RR=1.65, 95% CI=0.89-3.04) and no significant differences were observed between the two groups.

Risk of bias summary: Authors' judgments on each risk of bias item for each included study.

Study flow diagram.
Summary of the included studies. All were phase II clinical trials.
Discussion
BTCs are a heterogeneous group of aggressive malignancies comprising iCCA, eCCA, GBC and AVC, according to anatomical location. Although each subtype presents distinct biology, risk factors, molecular pathogenesis, prognosis, therapeutic options and epidemiology, RCTs often include patients affected by all these anatomical subtypes, which is a problematic issue in interpreting results.
The advent and the development of comprehensive whole-exome and transcriptome sequencing has led to a growing pharmaceutical and scientific interest in developing targeted agents in BTC. In this landscape, promising molecular targets for precision medicine in advanced BTC have been evaluated and are currently under investigation, representing a new option for a proportion of selected candidates (21). Between the novel treatments explored in RCTs, in recent years several EGFR-targeted therapies (single-agent or in addition to CHT) have been tested in various trials, failing to produce promising results (33-37).

Forest plot of comparison between gemcitabine (Gem)-based chemotherapy (CHT) plus anti-epidermal growth factor receptor (EGFR) versus gemcitabine-based chemotherapy alone; the outcome was hazard ratio of overall survival. CI: Confidence intervaI.
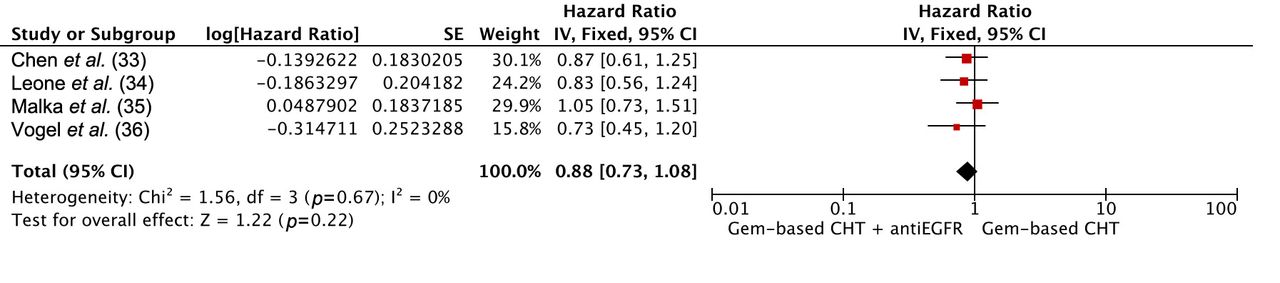
Forest plot of comparison between gemcitabine (Gem)-based chemotherapy (CHT) plus anti-epidermal growth factor receptor (EGFR) versus gemcitabine-based chemotherapy alone; the outcome was hazard ratio of progression-free survival. CI: Confidence intervaI.

Forest plot of comparison between gemcitabine (Gem)-based chemotherapy (CHT) plus anti-epidermal growth factor receptor (EGFR) versus gemcitabine-based chemotherapy alone; the outcome was risk ratio of objective response rate. CI: Confidence interval.
Our meta-analysis especially focused on the efficacy and safety of gemcitabine-based CHT plus EGFR-mAbs. The results of our meta-analysis confirmed no beneficial OS, PFS and ORR was observed in the pooled analysis with the addition of EGFR-targeted therapy to first-line CHT. As regards PFS, the absence of heterogeneity in the overall analysis for PFS suggested that the lack of efficacy was not dependent on the regimen used. Our results were in line with similar meta-analyses performed by Cai et al. (44) and Zhuang et al. (45), in which the authors detected a remarkable superiority of ORR, although this finding did not translate into a PFS and OS benefit. However, in contrast to their analyses, we included only the results of RCTs on gemcitabine-based CHT plus EGFR-mAbs excluding EGFR-TKIs. Of note, Cai et al. and Zhuang et al. did not find significant differences comparing grade 3-4 adverse events in either group.
In our analysis, we pooled five types of grade 3-4 ADEs. While no significant differences were found in the incidence of diarrhea and fatigue, the pooled data illustrated that more statistically significant hematological toxicities occurred in the CHT plus targeted therapy arm than in the one treated with CHT alone.

Forest plot of comparison between gemcitabine (Gem)-based chemotherapy (CHT) plus anti-epidermal growth factor receptor (EGFR) versus gemcitabine-based chemotherapy alone; the outcome was risk ratio of neutropenia. CI: Confidence interval.

Forest plot of comparison between gemcitabine (Gem)-based chemotherapy (CHT) plus anti-epidermal growth factor receptor (EGFR) antibodies versus gemcitabine-based chemotherapy alone; the outcome was risk ratio of thrombocytopenia. CI: Confidence interval.
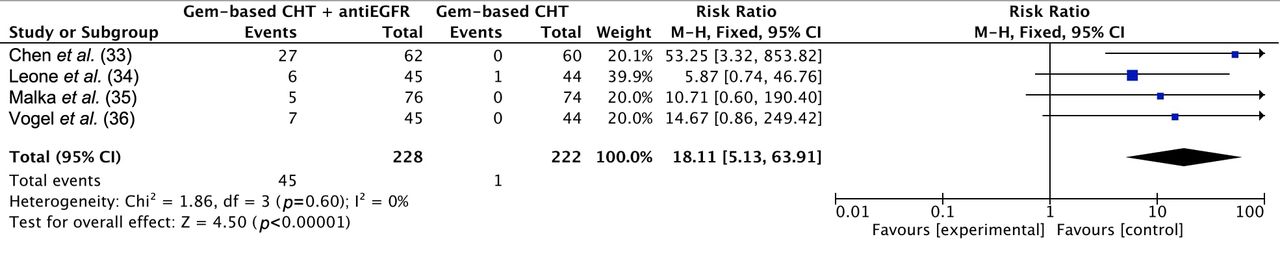
Forest plot of comparison between gemcitabine (Gem)-based chemotherapy (CHT) plus anti-epidermal growth factor receptor (EGFR) antibodies versus gemcitabine-based chemotherapy alone; the outcome was risk ratio of skin rash. CI: Confidence interval.

Forest plot of comparison between gemcitabine (Gem)-based chemotherapy (CHT) plus anti-epidermal growth factor receptor (EGFR) antibodies versus gemcitabine-based chemotherapy alone; the outcome was risk ratio of diarrhea. CI: Confidence interval.

Forest plot of comparison between gemcitabine (Gem)-based chemotherapy (CHT) plus anti-epidermal growth factor receptor (EGFR) antibodies versus gemcitabine-based chemotherapy alone; the outcome was risk ratio of fatigue. CI: Confidence interval.
The same results were found in the incidence of skin rash, a frequently observed grade 3-4 ADE in the group treated with gemcitabine-based CHT plus EGFR-mAbs. In lung cancer, skin rash occurrence is considered a strong predictor of outcome in patients treated with EGFR-targeted therapy on the basis of its association with reduced risk of death and increased chance of response (46,47). A recent meta-analysis analyzed data from 14 RCTs on anti-EGFR treatment and skin rash in biliary tract cancer (48); in this study, a longer OS (HR=0.47, 95% CI=0.31-0.71, p=0.0003) and PFS (HR=0.51, 95% CI=0.36-0.72, p=0.0001) was described in patients with higher grades of skin rash when compared with patients who received the same treatment but had lower grades or no skin rash. To date, the predictive role of skin rash for BTC patients receiving EGFR-targeted agents is not defined.
There are several limitations which might have influenced the results of this meta-analysis.
Firstly, only four RCTs were included, with small sample sizes, and all the included studies were industry funded. Secondly, two types of gemcitabine-based schedules and two different types of EGFR-mAbs (cetuximab and panitumumab) were included. Additionally, the meta-analyses included two RCTs (33, 35) with molecularly unselected patients, regardless of KRAS status, which would have a non-negligible effect on results.
Moreover, given the well-known biological heterogeneity of anatomical subtypes included in BTC, the inclusion of tumors arising from the biliary tree together with GBC and AVC might meaningfully influence the possibility of recognizing a survival benefit. This long-standing issue in the interpretation and generalizability of RCTs on BTC may be surmounted only through a more accurate selection of patients in future prospective trials.
In the current era of precision oncology, a mandatory point would be to better define genes and pathways involved in BTC to provide a deeper understanding of biological mechanisms underlying iCCA, eCCA, GBC and AVC. Progress in the management of BTC will necessarily have to pass through a close collaboration between molecular biology and clinical oncology in order to modify the natural history of this increasingly frequent, highly lethal, disease.
Conclusion
On the basis of this meta-analysis, the addition of EGFR-mAbs to gemcitabine-based first-line CHT in advanced BTC does not result in a statistically significant benefit in OS, PFS and ORR with increased grade 3-4 toxicity, and thus these agents should not be adopted into clinical practice. Further exploration of tumor biology and genetic aberrations in BTC is needed to improve patient outcomes that remain unsatisfactory.
Acknowledgements
The Authors received no financial support for the research, authorship, or publication of this article.
Footnotes
Authors' Contributions
Rizzo A: Made substantial contributions to conception of the study, analyzed the data and drafted the article; Frega G: made substantial contributions to conception of the study and gave final approval of the version to be published; Ricci AD: made substantial contributions to conception of the study, analyzed the data and was involved in revising the article critically for important intellectual content; Palloni A: helped to draft and revise the article; Abbati F: helped to draft and revise the article; De Lorenzo S: revised the article; Deserti M: revised the article; Tavolari S: made substantial contributions to conception of the study and revised the article; Brandi G: was involved in revising the article critically for important intellectual content and gave final approval of the version to be published. All Authors critically revised the article, approved the final version to be published, and agree to be accountable for all aspects of the work.
This article is freely accessible online.
Conflicts of Interest
The Authors state that they have no conflicts of interest in regard to this study.
- Received November 6, 2019.
- Revision received November 12, 2019.
- Accepted November 18, 2019.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The (Eternal) Debate on Microwave Ablation Versus Radiofrequency Ablation in BCLC-A Hepatocellular Carcinoma
- Circulating Tumor DNA in Biliary Tract Cancer: Current Evidence and Future Perspectives
- How to Choose Between Percutaneous Transhepatic and Endoscopic Biliary Drainage in Malignant Obstructive Jaundice: An Updated Systematic Review and Meta-analysis
- Second-line Treatment in Advanced Biliary Tract Cancer: Today and Tomorrow