Article Text

Abstract
Background: Although circulating tumour DNA has been detected in patients with different types of cancer, little is known of free RNA in cancer patients.
Aims: We investigated the presence of RNA from epithelial tumours in plasma from patients with colorectal carcinomas, and its correlation with tumour characteristics and circulating tumour cells.
Methods: β-actin mRNA was analysed to assess the viability of plasma RNA in samples from 53 patients with colonic cancer and 25 controls. Subsequently, nested primers were used to detect the presence of cytokeratin 19 (CK19) and carcinoembryonic antigen (CEA) RNA in the same samples. Nine clinicopathological parameters were studied to correlate the molecular and clinical parameters. Additionally, we investigated for micrometastases in blood in 18 of these patients and in 10 of the controls samples.
Results: All samples had detectable quantities of β-actin RNA. In the controls, one case (4%) was positive for CEA and five (20%) for CK19 RNA; of the 53 patients, 17 cases (32%) were positive for CEA and 39 (73.6%) for CK19 RNA. This was statistically significant (p=0.000001). Advanced stages (p=0.03) and soluble CEA status (p=0.03) were associated with the presence of CEA, CK19, or both RNAs in plasma. Lymph node metastases (p=0.06) and vascular invasion (p=0.07) were almost significant. On the basis of these results, we examined the possible presence of micrometastases in blood in several of these patients. The presence of plasma tumour RNA was found to be associated with circulating tumour cells in blood (p=0.04).
Conclusions: Epithelial tumour RNA is detectable in plasma from colon cancer patients. This molecular event is associated with advanced stages and circulating tumour cells. Our results could offer new approaches in the diagnosis and monitoring of colon cancer.
- colon cancer
- plasma RNA
- advanced stages
- tumour cells
- genetic markers
- CK19, cytokeratin 19
- CEA, carcinoembryonic antigen
- MNC, mononuclear blood cells
- MEIA, microparticle enzyme immunoassay
- dNTP, deoxynucleotide triphosphate
- MNC, mononuclear cells
- RT-PCR, reverse transcription-polymerase chain reaction
Statistics from Altmetric.com
- CK19, cytokeratin 19
- CEA, carcinoembryonic antigen
- MNC, mononuclear blood cells
- MEIA, microparticle enzyme immunoassay
- dNTP, deoxynucleotide triphosphate
- MNC, mononuclear cells
- RT-PCR, reverse transcription-polymerase chain reaction
Colon cancer is one of the most common malignancies in western countries and represents the second cause of death from cancer.1 Survival is directly related to the pathological stage with a dramatic drop between early and advanced stages.2 Currently, diagnosis is based on histological study but more refined molecular techniques can contribute towards optimising the pathological classification.3
Many genetic alterations have been found during the development and progression stages of colon cancer, including germline and somatic mutations in different genes (oncogenes, tumour suppressor genes, and mismatch repair genes).4 More recently it has been demonstrated that some of these molecular changes, mainly oncogene and tumour suppressor gene mutations, can be detected in the plasma and serum of patients with colorectal cancer.5–8 Similarly, these alterations, and others in several microsatellites, have been observed in patients with many other malignancies, such as melanomas, and lung, breast, head and neck, pancreatic, and renal carcinomas.9–17 The prognostic implications of circulating plasma DNA in patients with malignancies regarding the outcome of the disease is currently undergoing evaluation, although a correlation with poor survival in pancreatic carcinomas has been reported.12 A new recently published plasma DNA utility with tumour DNA features has been used as a method of screening for somatic mutations frequently found in tumours with the objective of detecting these alterations in the preclinical phase of the disease.18
Characterisation of plasma DNA as tumour DNA depends on the alteration rate of a specific marker in tumour DNA and the sensitivity of the procedure used to detect it in plasma DNA. This strategy justifies the use of several molecular markers to increase the number of cases identified with positive circulating DNA. However, new approaches with RNA based amplification methods could offer greater levels of specificity and sensitivity. The same method used to detect circulating cancer cells19–22 can be applied to investigate free RNA in the plasma of cancer patients. Although it has been proposed that RNA is more breakable than DNA because of supposed susceptibility to degradation by blood RNases, circulating RNA in melanoma23 and breast cancer patients24 has recently been detected despite the fact, as was reported, that blood RNases are possibly increased in patients with malignancies.25 The fact that extracellular RNA exists with sufficient integrity as to allow reverse transcription-polymerase chain reaction (RT-PCR) amplification represents a new tool in the strategy to determine nucleic acids in the plasma of cancer patients and their value as prognostic factors.
The present study was performed on the basis of these facts using two mRNA markers, cytokeratin 19 (CK19) and carcinoembryonic antigen (CEA), which have demonstrated ability in detecting circulating colon cancer cells, to investigate: (a) the presence at diagnosis of detectable RNA of epithelial origin in the plasma of colon cancer patients, (b) the distribution of nine clinicopathological parameters in patients with and without epithelial RNA in plasma, and (c) the association between the presence of the two mRNA markers in plasma and circulating tumour cells.
METHODS
Plasma samples and RNA extraction
Informed consent was obtained from all participants following an explanation of the nature of the study, as approved by the research ethics board of our hospital. Between October 1999 and June 2000, blood samples from 53 patients with colorectal carcinoma were collected preoperatively at the time of surgery. Plasma was prepared by centrifugation of peripheral blood at 1000 g for 10 minutes followed by careful aliquoting. Samples were snap frozen at −80°C until processing. Blood samples were also obtained from 25 healthy controls.
RNA was extracted from 3 ml of plasma using a commercial kit according to the manufacturer's protocol (Rneasy Mini Kit; Qiagen Inc., Hilden, Germany) with the following modifications: 3 ml plasma samples were mixed with 600 μl buffer RLT and 6 μl β-mercaptoethanol. Subsequently, 3.5 ml ethanol 70% was added and cooled to 4°C for 30 minutes. A final centrifugation was performed at 1500 g for five minutes and the supernatant was collected. One column was used repeatedly until the whole sample had been processed. The final elution volume was 50 μl and the concentration of RNA was approximated by spectrophotometry.
Circulating tumour cell analysis
The study of micrometastases in blood was performed in three steps. Firstly, 10 ml of blood were taken from 18 patients and 10 controls; mononuclear cells (MNC) were obtained from these samples using a Ficoll solution (Lymphoprep; Nycomed Pharma AS, Oslo, Norway). Secondly, the MNC fraction in epithelial circulating tumour cells was enriched by a positive isolation method (Dynabeads epithelial enrich protocol; Dynal AS, N-0212 Oslo, Norway).26,27 Briefly, the MNC fraction was mixed with magnetic polystyrene beads coated with a IgG1 monoclonal antibody specific for two glycopolypeptide membrane antigens expressed on most normal and neoplastic human epithelial tissues. During the incubation period, the epithelial cells bind to magnetic beads and, subsequently, the rosetted cells can be isolated and washed using a magnet. As a result, the circulating tumour cells were enriched by more than 3 logs from MNC. Finally, RNA was extracted using the aforementioned commercial Rneasy Mini Kit.
Clinicopathological parameters analysed
A correlation study was designed with the aim of investigating the prognostic value of the following parameters obtained from the medical records of the patients: birth date, sex, tumour location, tumour size, lymph node metastases, vascular invasion, pathological stage, histological grade, and CEA levels. CEA levels were determined by a microparticle enzyme immunoassay method (AxSYM CEA; Abbott, Wiesbaden, Germany) and the normal range was 0–5 ng/ml.
RT-PCR and primers condition
RNA from plasma and cells was subjected to reverse transcription and amplified using the GeneAmp gold RNA PCR Core Kit for RT-PCR (PE Biosystems, Foster City, California, USA) by incubation at 42°C for 12 minutes and then undergoing a 43 cycle PCR with variable annealing temperatures depending on the pair primers. A mixture was prepared consisting of 5.5 μl of ARN (5–15 ng), 2 μl 5× RT-PCR buffer, 0.7 μl 25 mM magnesium chloride, 0.8 μl of 10 mM deoxynucleotide triphosphate (dNTP) blend, 2 units of RNAase inhibitor, 0.5 μl of 100 mM DTT, 0.5 units of AmpliTaq Gold DNA Polymerase, 3 units of MultiScribe Reverse Transcriptase, and 0.6 μM of specific reverse primers. The final reaction volume was 10 μl. Amplification was performed in a thermal cycler (Perkin-Elmer, Cetus, Foster City, California, USA).
Three human genes were amplified using the above protocol, β-actin, CK19, and CEA. A second nested PCR was performed because the signal obtained from plasma ARN was weak. β-actin was used to verify the presence and integrity of serum RNA (as it is expected to be expressed in all individuals) because storage can modify the results.23
β-actin primers
Bf (outer, sense) 5`CCAACCGCGAGAAGATGACC3`; Br (outer, antisense) 5`TGCCAATGGTGATGACCTGG3`. Bnf (nested, sense) 5`GATCATGTTTGAGACCTTC3`; Bnr (nested, antisense) 5`GTCAGGCAGCTCGTAG3`; PCR conditions for outer primers were 95°C for nine minutes followed by 40 cycles of 95°C for 20 seconds, 64°C for 15 seconds, and 72°C for 30 seconds, and finally 72°C for 11 minutes. Nested PCR conditions were 95°C for nine minutes followed by 40 cycles of 95°C for 30 seconds, 60°C for 30 seconds, and 72°C for 30 seconds, and finally 72°C for 11 minutes.
CK19 primers
The CK19 nested primers are designed to maximise mismatch between the CK19 gene and the two processed pseudogenes (Dynal CK 19 nested primers; Dynal AS, N-0212 Oslo, Norway). CKf (outer, sense) 5`GTGGAGGTGGATTCCGCTCC3`; CKr (outer, antisense) 5`TGGCAATCTCCTGCTCCAGC3`. CKnf (nested, sense) 5`ATGGCCGAGCAGAACCGGAA3`; CKnr (nested, antisense) 5`CCATGAGCCGCTGGTACTCC3`. PCR conditions for outer primers were 95°C for nine minutes followed by 43 cycles of 95°C for 30 seconds, 58°C for 30 seconds, and 72°C for one minute, and finally 72°C for 11 minutes. Nested PCR conditions were 95°C for nine minutes followed by 40 cycles of 95°C for 30 seconds, 61°C for 30 seconds, and 72°C for 30 seconds, and finally 72°C for 11 minutes.
CEA primers
CEA1, 5`TCTGGAACTTCTCCTGGTCTCTCAGCTGG3`; CEA2, 5`TGTAGCTGTTGCAAATGCTTTAAGGAAGAAGC3`; CEA3, 5`GGGCCACTGTCGGCATCATGATTGG3`. The first PCR used primers CEA1 and CEA2; nested PCR used primers CEA3 and CEA2. Conditions for outer primers and nested primers were 95°C for nine minutes followed by 40 (outer) or 25 (nested) cycles of 95°C for 30 seconds, 65°C for 30 seconds, and 72°C for one minute, and finally 72°C for 11 minutes. Nested PCR was amplified using 1.2 μl from the first PCR amplification in a final volume of 10 μl in the presence of 0.30 units of AmpliTaq Gold DNA Polymerase (Perkin-Elmer, Roche Molecular Systems, Inc., Branchburg, New Jersey, USA), 1 μl of 10× PCR buffer, 200 μM dNTP, 0.6 μM of each primer, and different concentrations of MgCl2, depending on the polymorphic marker.
A nested PCR was necessary to obtain clear results from low quantities of plasma RNA. Nested PCR is a very sensitive technique capable of detecting minimal amounts of specific mRNA in plasma. Increasing the number of PCR cycles can also offer positive results in controls. Therefore, all nested amplification conditions were designed to avoid this latter event. RT-PCR amplifications included a positive and negative control (CEA or CK19) consisting of RNA from colon tumour tissue and lymphocytes. All RT-PCR amplifications were performed with particular attention being paid to preventing contamination that can falsify the results when low quantities of RNA are analysed. The risk of contamination yielding false positive results was further minimised by repeating the assay using previously prepared plasma aliquots.
Detection
The final 10 μl of the PCR product was mixed with a 3 μl volume of loading buffer (total volume 13 μl), 0.02% xylene cyanol, and 0.02% bromophenol blue. Electrophoresis was run on non-denaturing 8–12% polyacrylamide gels for two hours at 500 V. After gel electrophoresis, the band intensity was detected by a non-radioisotopic technique using a commercially available silver staining method.28 Band intensities were analysed by densitometry. The gel image was captured by a GS-690 Imaging Densitometer (Bio-Rad Laboratories, Hercules, California, USA), digitised at 400 dpi, and analysed using Multi-Analyst/PC (Bio-Rad Laboratories, Hercules, California, USA).
Statistical analysis
The variables analysed were contrasted using the χ2 test, and with the χ2 test with Yates' correction or Fisher's exact test when any of the expected frequencies were less than 5. Two tailed p values <0.05 were considered statistically significant. Statistical analyses were performed using the EPI-INFO package, version 6.04.
RESULTS
When the viability of the RNA samples was analysed through amplification of β-actin, it was found that all plasma samples from controls and patients had detectable quantities of β-actin mRNA, demonstrating an acceptable integrity to amplification (fig 1).
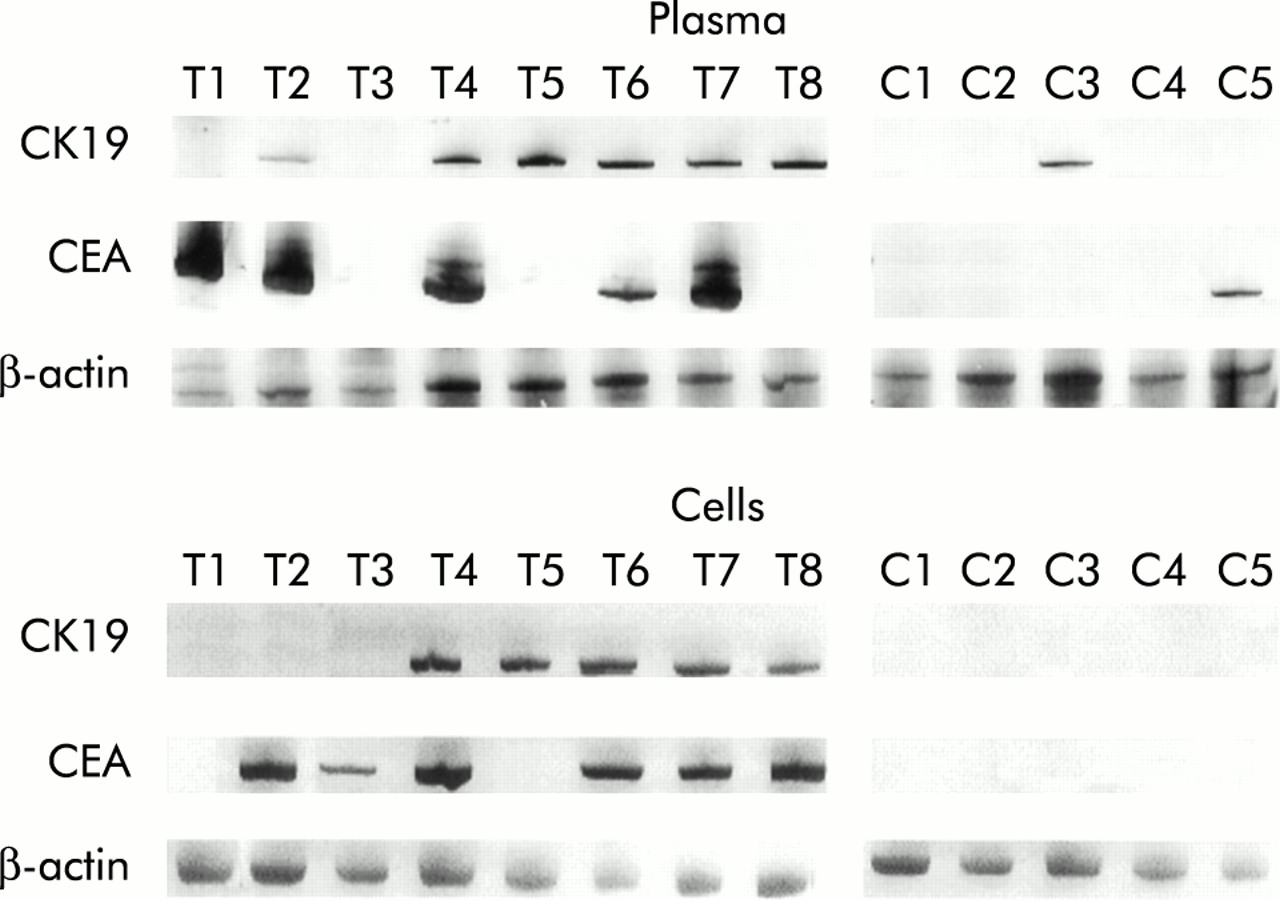
{kind=link}
Nested reverse transcription-polymerase chain reaction of carcinoembryonic antigen (CEA) and cytokeratin 19 (CK19) mRNA in plasma and circulating cells of controls (C) and patients with colorectal cancer (T). Six patients (T2, T4–T8) are shown with at least one positive marker in plasma and cells. One patient (T3) displayed a positive mRNA marker only in cells and one patient (T1) revealed a positive mRNA marker only in plasma. β-actin showed that all samples displayed detectable plasma and circulating cell RNA.
Subsequently, the presence of detectable quantities of CEA and CK19 mRNA in plasma samples was assessed. It was found that one (4%) of the control samples was positive for CEA mRNA. When the same study was performed in plasma mRNA from tumour patients, 17 of 53 (32%) were positive. Analysis of CK19 mRNA displayed the presence of CK19 in five of 25 controls (20%), while in plasma mRNA from patients, 39 of 53 samples (73.6%) showed the presence of CK19 mRNA (fig 1).
When the distribution of these epithelial mRNA markers in the plasma of controls and patients was analysed it was observed that six (24%) of the controls were positive for at least one marker, and the remaining 19 (76%) samples were negative for both markers. In contrast, 44 (83%) patients were found to be positive for at least one marker, and nine (17%) were negative for both epithelial markers. This distribution displayed a statistically significant association (p=0.000001) (table 1).
Distribution of mRNA epithelial markers (cytokeratin 19 and carcinoembryonic antigen) in controls and patients
When the nine clinicopathological parameters were compared with the molecular results, four showed a consistent relation to the presence of epithelial tumour mRNA in one or both of the markers used (CK19, CEA). The tumour characteristics that displayed a statistically significant difference were advanced pathological stage (p=0.03) and soluble CEA levels (p=0.03); the parameters close to significance were lymph node metastases (p=0.06) and vascular invasion (p=0.07) (table 2). None of the remaining clinicopathological parameters demonstrated statistically significant differences. Additionally, among the 38 patients with available determination of serum CEA glycoprotein, 26 (68.5%) cases showed a correlation between plasma mRNA CEA and CEA glycoprotein.
Distribution of several clinicopathological parameters and levels of soluble carcinoembryonic antigen (CEA) in relation to the presence of mRNA markers in plasma
Based on this association of epithelial mRNA marker in plasma and advanced stages, we looked for circulating tumour cells in several of these patients and controls. None of the 10 controls tested displayed the presence of epithelial mRNA in MNC. On the other hand, 13 (72%) of the MNCs from the 18 patients analysed were positive for the markers studied, seven with CK19 and six with both markers. When the results obtained in plasma and MNC in patients were compared, 12 (92%) of 13 patients with circulating tumour cells showed the presence of epithelial mRNAs in plasma. This result demonstrated a statistically significant association (p=0.04) (table 3).
Distribution of epithelial mRNA markers in plasma versus circulating tumour cells in patients
DISCUSSION
The use of a simple blood test in clinical oncology for the detection of sporadic cancer is perceived as a possible goal in the near future. Improvements in molecular and genetic approaches have permitted the identification of tumour derived nucleic acids circulating in the plasma of cancer patients.7–18 The origin and release mechanisms of these nucleic acids into plasma, and the protection of DNases and RNases action, are unknown. The most common hypothesis is that they come from lysis of circulating cancer cells or micrometastases shed by the tumour as well as from tumour necrosis, apoptosis, and active release.29 Additionally, nucleic acids have been found on the surface of cancer cells30,31 and they could be shed within vesicles bound to protein or phospholipid, thus being protected against action.32,33
While circulating tumour derived DNA has been widely studied in the majority of cancer types, current knowledge of the second nucleic acid RNA is scarce. Only three experiences of mRNA detection in cancer patients and controls have been reported.23,24,34 The study by Lo and colleagues34 detected Epstein-Barr virus associated RNA in the plasma of patients with nasopharyngeal carcinomas. However, even though it is a good example of specific mRNA expression in a malignancy, the use of RNA of virus tumour associated as a positive detection marker is restricted to those uncommon tumours with a demonstrated relation to a virus, such as nasopharyngeal or cervical carcinomas. The two other original works reported detection of specific mRNA from tumour tissues in the RNA of plasma in patients with metastatic melanoma and breast carcinoma.23,24 These studies, similar to those that investigated circulating tumour cells in minimal residual disease,19–22 demonstrated that it is possible to find free tumour mRNA in the plasma of patients with cancer, which indicates that other tumours could also be studied if suitable mRNA markers were available.
The present series analysed patients with colon cancer at several stages, and also attempted to identify cases with circulating tumour mRNA using two specific epithelial markers. Our results offer evidence for mRNA of tumour origin in the plasma of colon cancer patients, with a consistent statistically significant difference compared with normal controls. Additionally, when we examined the correlation between the presence of epithelial mRNA in the plasma of these patients and their clinicopathological characteristics, we found that advanced pathological stage was significantly prevalent in cases with one or both positive epithelial markers, and vascular invasion and lymph node metastases were close to being significant. No data on clinicopathological and molecular correlations are available.
However, based on these results and previously reported findings regarding plasma tumour mRNA in metastatic melanoma,23 we hypothesise that, at least in colon cancer patients, the presence of circulating tumour mRNA could be a prognostic factor linked to micrometastases in blood. When this possibility was examined, we observed that 92% of patients showing circulating epithelial tumour cells displayed the same positive RNA markers in plasma. This is the first study to demonstrate the close relationship between circulating tumour cells and circulating tumour RNA. Additionally, two patients with no evidence of disseminated disease had a positive epithelial marker in plasma. This may be explained by minimal illegitimate levels of CK19 mRNA expression in mononuclear blood cells35 and increased levels of CEA in almost 30% of smokers.36 In the same way, we found that 4% and 20% of controls had mRNA of CEA and CK19 in plasma, respectively. Alternatively, it could be that the enrichment in nucleic acids from tumour improves the detection capability, making the plasma study method more sensitive than others in the detection of disseminated disease.
Additionally, we would like to point out that the rate of identification of circulating tumour cells in our patients was higher than expected, but several facts may explain these results: (a) we used a circulating tumour cell enrichment protocol previous to RNA extraction, (b) two markers were used in a very sensitive nested PCR, and (c) the subset of 13 patients had advanced stage of disease (eight with stage C and five with stage B2).
In conclusion, specific determination of mRNA of epithelial origin in the plasma of patients with colon cancer is a reality. Moreover, a positive correlation with pathological parameters compatible with more aggressive tumours and circulating tumour cells was observed in patients with tumour mRNA present in plasma. Further studies in other malignancies are needed to address the potential of this new molecular marker in situations such as cancer diagnosis, monitoring the outcome of disease, and eventually as a treatment response indicator.
Acknowledgments
We would like to express our gratitude to the patients that participated in the study and thank Martin Hadley-Adams for revision and preparation of the manuscript. Supported by grants from: FIS 01/0505; Fundación Caja Madrid; AECC; and Aventis Pharma.