Apoptosis-Inducing Factor, Mitochondrion-Associated 3 (AIFM3) Protein Level in the Sera as a Prognostic Marker of Cholangiocarcinoma Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Sera from CCA Patients and HC
2.3. Prediction of Secretory Proteins
2.4. Western Blot Analysis
2.5. Dot Blot Assay and Data Acquisition
2.6. Statistical Analysis
3. Results
3.1. Bioinformatic Analysis of AIFM3 Protein to Predict its Secretory Protein Nature
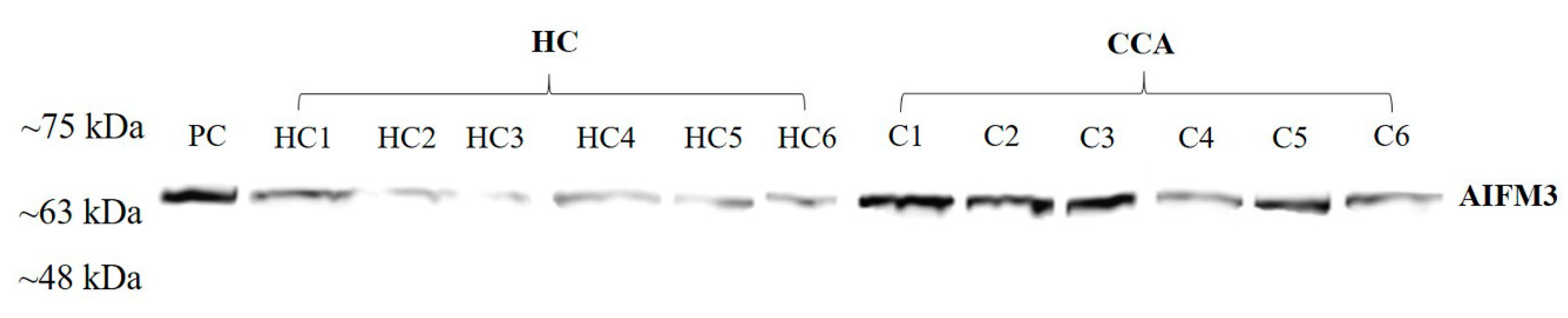
3.2. AIFM3 Expression in the Serum Samples
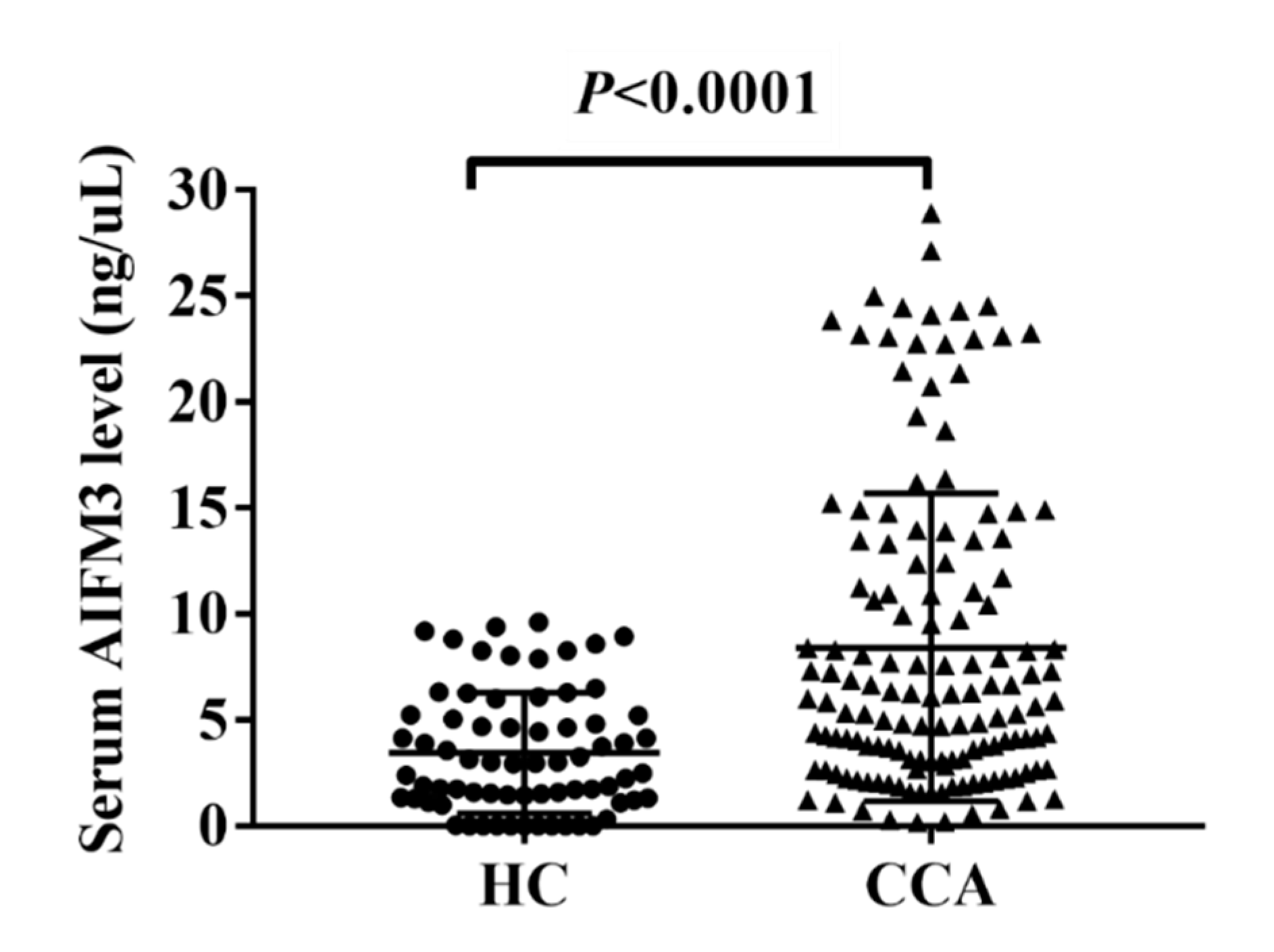
3.3. Serum AIFM3 Levels of CCA and HC
3.4. Correlation between AIFM3 Expression in Serum and CCA Tissues
3.5. The Correlation of Serum AIFM3 Levels with Clinical Parameters
3.6. Evaluation of the Prognostic Potential of Serum AIFM3 in Comparison with other Prognostic Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blechacz, B.; Gores, G.J. Cholangiocarcinoma: Advances in pathogenesis, diagnosis, and treatment. Hepatology 2008, 48, 308–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erice, O.; Merino-Azpitarte, M.; Arbelaiz, A.; Gutierrez-Larranaga, M.; Jimenez-Aguero, R.; Perugorria, M.J.; Bujanda, L.; Banales, J.M. Molecular Mechanisms of Cholangiocarcinogenesis: New Potential Targets for Therapy. Curr. Drug Targets 2017, 18, 932–949. [Google Scholar] [CrossRef] [PubMed]
- Razumilava, N.; Gores, G.J.; Lindor, K.D. Cancer surveillance in patients with primary sclerosing cholangitis. Hepatology 2011, 54, 1842–1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, S.L.; Sachdeva, A.; Garcea, G.; Gravante, G.; Metcalfe, M.S.; Lloyd, D.M.; Berry, D.P.; Dennison, A.R. Elevation of carbohydrate antigen 19.9 in benign hepatobiliary conditions and Its correlation with serum bilirubin concentration. Digest Dis. Sci. 2008, 53, 3213–3217. [Google Scholar] [CrossRef] [PubMed]
- Silsirivanit, A.; Araki, N.; Wongkham, C.; Pairojkul, C.; Narimatsu, Y.; Kuwahara, K.; Narimatsu, H.; Wongkham, S.; Sakaguchi, N. A novel serum carbohydrate marker on mucin 5AC: Values for diagnostic and prognostic indicators for cholangiocarcinoma. Cancer 2011, 117, 3393–3403. [Google Scholar] [CrossRef]
- Liu, S.L.; Song, Z.F.; Hu, Q.G.; Shan, D.; Hu, S.B.; Li, J.; Zheng, Q.C. Serum carbohydrate antigen (CA)19-9 As prognostic factor in cholangiocarcinoma: A meta-analysis. Front. Med. China 2010, 4, 457–462. [Google Scholar] [CrossRef]
- Juntermanns, B.; Radunz, S.; Heuer, M.; Hertel, S.; Reis, H.; Neuhaus, J.P.; Vernadakis, S.; Trarbach, T.; Paul, A.; Kaiser, G.M. Tumor markers as a diagnostic key for hilar cholangiocarcinoma. Eur. J. Med. Res. 2010, 15, 357–361. [Google Scholar] [CrossRef] [Green Version]
- Xie, Q.; Lin, T.; Zhang, Y.; Zheng, J.; Bonanno, J. Molecular cloning and characterization of a human AIF-like gene with ability to induce apoptosis. J. Biol. Chem. 2005, 280, 19673–19681. [Google Scholar] [CrossRef] [Green Version]
- Chua-On, D.; Proungvitaya, T.; Techasen, A.; Limpaiboon, T.; Roytrakul, S.; Wongkham, S.; Wongkham, C.; Somintara, O.; Sungkhamanon, S.; Proungvitaya, S. High expression of apoptosis-inducing factor, mitochondrion-associated 3 (AIFM3) in human cholangiocarcinoma. Tumour Biol. 2016, 37, 13659–13667. [Google Scholar] [CrossRef]
- Zheng, A.; Zhang, L.; Song, X.; Wang, Y.; Wei, M.; Jin, F. Clinical implications of a novel prognostic factor AIFM3 in breast cancer patients. BMC Cancer 2019, 19, 451. [Google Scholar] [CrossRef] [Green Version]
- Dupont, W.D.; Plummer, W.D., Jr. Power and sample size calculations. A review and computer program. Control Clin. Trials 1990, 11, 116–128. [Google Scholar] [CrossRef]
- Petersen, T.N.; Brunak, S.; von Heijne, G.; Nielsen, H. SignalP 4.0: Discriminating signal peptides from transmembrane regions. Nat. Methods 2011, 8, 785–786. [Google Scholar] [CrossRef] [PubMed]
- Bendtsen, J.D.; Jensen, L.J.; Blom, N.; Von Heijne, G.; Brunak, S. Feature-based prediction of non-classical and leaderless protein secretion. Protein Eng. Des. Sel. 2004, 17, 349–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanjappa, V.; Thomas, J.K.; Marimuthu, A.; Muthusamy, B.; Radhakrishnan, A.; Sharma, R.; Khan, A.A.; Balakrishnan, L.; Sahasrabuddhe, N.A.; Kumar, S.; et al. Plasma Proteome Database as a resource for proteomics research: 2014 update. Nucl. Acids Res. 2014, 42, D959–D965. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.C.; Berkelman, T.; Yadav, G.; Hammond, M. A defined methodology for reliable quantification of Western blot data. Mol. Biotechnol. 2013, 55, 217–226. [Google Scholar] [CrossRef] [Green Version]
- Fang, R.; Wey, A.; Bobbili, N.K.; Leke, R.F.G.; Taylor, D.W.; Chen, J.J. An analytical approach to reduce between-plate variation in multiplex assays that measure antibodies to Plasmodium falciparum antigens. Malar. J. 2017, 16, 287. [Google Scholar] [CrossRef] [Green Version]
- Budczies, J.; Klauschen, F.; Sinn, B.V.; Gyorffy, B.; Schmitt, W.D.; Darb-Esfahani, S.; Denkert, C. Cutoff Finder: A comprehensive and straightforward Web application enabling rapid biomarker cutoff optimization. PLoS ONE 2012, 7, e51862. [Google Scholar] [CrossRef] [Green Version]
- Chistiakov, D.A.; Myasoedova, V.A.; Grechko, A.V.; Melnichenko, A.A.; Orekhov, A.N. New biomarkers for diagnosis and prognosis of localized prostate cancer. Semin. Cancer Biol. 2018, 52, 9–16. [Google Scholar] [CrossRef]
- Rabouille, C. Pathways of Unconventional Protein Secretion. Trends Cell. Biol. 2017, 27, 230–240. [Google Scholar] [CrossRef]
- Fernandez-Pol, J.A.; Hamilton, P.D.; Klos, D.J. Genomics, Proteomics and Cancer: Specific ribosomal, mitochondrial, and tumor reactive proteins can be used as biomarkers for early detection of breast cancer in serum. Cancer Genom.-Proteom. 2005, 2, 1–24. [Google Scholar]
- Jubran, R.; Kocsis, J.; Garam, N.; Malati, E.; Gombos, T.; Barabas, L.; Graf, L.; Prohaszka, Z.; Fishelson, Z. Circulating mitochondrial stress 70 protein/mortalin and cytosolic Hsp70 in blood: Risk indicators in colorectal cancer. Int. J. Cancer 2017, 141, 2329–2335. [Google Scholar] [CrossRef] [Green Version]
- Sanmai, S.; Proungvitaya, T.; Limpaiboon, T.; Chua-On, D.; Seubwai, W.; Roytrakul, S.; Wongkham, S.; Wongkham, C.; Somintara, O.; Sangkhamanon, S.; et al. Serum pyruvate dehydrogenase kinase as a prognostic marker for cholangiocarcinoma. Oncol. Lett. 2019, 17, 5275–5282. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, M.; Yaginuma, Y.; Hayashi, H.; Shimizu, T.; Endo, Y.; Taniguchi, N. Reactivity of a Monoclonal-Antibody to Manganese Superoxide-Dismutase with Human Ovarian-Carcinoma. Cancer Res. 1990, 50, 2538–2542. [Google Scholar] [CrossRef]
- Zhu, N.Q.; Hou, J.Y.; Wu, Y.H.; Liu, J.X.; Li, G.; Zhao, W.J.; Ma, G.Y.; Chen, B.; Song, Y.X. Integrated analysis of a competing endogenous RNA network reveals key lncRNAs as potential prognostic biomarkers for human bladder cancer. Medicine 2018, 97, e11887. [Google Scholar] [CrossRef]
- Teerlink, C.; Nelson, Q.; Burt, R.; Cannon-Albright, L. Significant evidence of linkage for a gene predisposing to colorectal cancer and multiple primary cancers on 22q11. Clin. Transl. Gastroenterol. 2014, 5, e50. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter (Normal Range) | HC (n = 70) | CCA (n = 141) | p-Value |
|---|---|---|---|
| Age | 41 ± 7 | 60 ± 6.5 a | * <0.001 |
| (19–85) | (31–76) | ||
| Total protein | NA | 7.5 ± 0.5 b | NA |
| (6.5–8.8 g/dL) | (4.6–10) | ||
| Total bilirubin | NA | 0.6 ± 0.8 b | NA |
| (0.25–1.5) | (0.2–24.9) | ||
| Direct bilirubin | NA | 0.3 ± 0.6 b | NA |
| (0–0.5 mg/dL) | (0–13.7) | ||
| ALT | 21 ± 6 | 38 ± 20 b | * <0.001 |
| (4–36 U/L) | (4–36) | (1–795) | |
| AST | 20 ± 4 | 40 ± 18.7 b | * <0.001 |
| (12–32 U/L) | (6–34) | (4–1112) | |
| ALP | 47 ± 9 | 168 ± 79 b | * <0.001 |
| (42–121 U/L) | (27–98) | (35–1068) | |
| Serum AIFM3 levels (ng/µL) | 3.258 ± 2.671 | 8.419 ± 7.269 c | * <0.001 |
| (0.001–9.602) | (0.175–28.907) | ||
| CA19-9 | NA | 67.7 ± 435.8 d | NA |
| (0–37 U/mL) | (0.6–1000) | ||
| CEA | NA | 5.1 ± 4.7 e | NA |
| (0–2.5 ng/mL) | (0.9–917.6) |
| Clinical Parameters | No. | Serum AIFM3 Levels (ng/µL) | ||
|---|---|---|---|---|
| ≤8.292 | >8.292 | p-Value a | ||
| Gender (n = 136) | ||||
| Male | 91 | 62 (45.5%) | 29 (21.3%) | 0.701 |
| Female | 45 | 26 (19.1%) | 19 (14.1%) | |
| Lymph node metastasis (n = 137) | ||||
| No | 62 | 50 (36.4%) | 12 (8.7%) | * 0.001 |
| Yes | 75 | 40 (29.1%) | 35 (25.8%) | |
| Age (Years) | 136 | 58.2 ± 9.5 | 63.2 ± 6.9 | * 0.002 b |
| (n = 89) | (n = 42) | |||
| Total protein (g/dL) | 131 | 7.3 ± 1.1 | 7.7 ± 0.8 | 0.094 |
| (n = 89) | (n = 42) | |||
| Total bilirubin (mg/dL) | 131 | 2.1 ± 4.1 | 1.3 ± 1.7 | 0.250 |
| (n = 89) | (n = 42) | |||
| Direct bilirubin (mg/dL) | 131 | 1.4 ± 2.6 | 0.9 ± 1.6 | 0.395 |
| (n = 89) | (n = 42) | |||
| ALT (U/L) | 131 | 69.7 ± 112.4 | 45.7 ± 38.9 | 0.475 |
| (n = 89) | (n = 42) | |||
| AST (U/L) | 131 | 88.6 ± 174.1 | 49.8 ± 38.2 | 0.624 |
| (n = 89) | (n = 42) | |||
| ALP (U/L) | 131 | 247.3 ± 191.7 | 209.9 ± 200.7 | 0.067 |
| (n = 89) | (n = 42) | |||
| Survival time (days) | 139 | 579.8 ± 649.6 | 358.0 ± 185.4 | * 0.017 b |
| (n = 87) | (n = 52) | |||
| Clinicopathological Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Lymph node metastasis | 1.13 (0.84–1.95) | 0.279 | 1.38 (0.96–2.14) | 0.103 |
| (non-metastasis or metastasis) | ||||
| Histological grading | 1.10 (0.56–1.21) | 0.567 | 0.99 (0.47–1.23) | 0.721 |
| (non-papillary or papillary) | ||||
| Gender (female or male) | 1.20 (0.71–1.65) | 0.731 | 1.35 (0.65–1.27) | 0.610 |
| Age (≤60 or >60 yr) | 1.07 (0.88–2.01) | 0.345 | 1.16 (0.61–2.21) | 0.442 |
| Total protein | 0.84 (0.56–1.24) | 0.239 | 0.95 (0.50–1.41) | 0.357 |
| (≤8.8 or >8.8 g/dL) | ||||
| Total bilirubin | 1.09 (0.64–1.88) | 0.704 | 1.42 (0.65–2.59) | 0.562 |
| (≤1.5 or >1.5 mg/dL) | ||||
| Direct bilirubin | 0.96 (0.67–1.59) | 0.847 | 0.78 (0.31–1.99) | 0.694 |
| (≤0.5 or >0.5 mg/dL) | ||||
| ALT (≤36 or >36 U/L) | 1.22 (0.90–2.02) | 0.265 | 1.44 (0.99–2.72) | 0.331 |
| AST (≤32 or >32 U/L) | 1.28 (0.94–1.81) | 0.546 | 1.07 (0.83–2.47) | 0.664 |
| ALP (≤121 or >121 U/L) | 1.30 (0.84–1.45) | 0.567 | 1.45 (0.97–2.49) | 0.704 |
| AIFM3 levels | 1.98 (1.28–3.26) | * 0.015 | 3.15 (1.92–6.37) | * 0.009 |
| (≤8.292 or >8.292 ng/µL) | ||||
| Tumor Markers | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| AIFM3 (cut-off 8.292 ng/µL) | 1.98 (1.28–3.26) | * 0.015 | 3.15 (1.92–6.37) | * 0.009 |
| CA19-9 (cut-off 900 U/mL) | 1.21 (0.61–2.50) | 0.361 | 1.39 (0.81–2.41) | 0.240 |
| CEA (cut-off 5.5 ng/mL) | 1.57 (1.02–2.40) | * 0.038 | 1.81 (0.90–3.25) | 0.088 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chua-on, D.; Proungvitaya, T.; Tummanatsakun, D.; Techasen, A.; Limpaiboon, T.; Roytrakul, S.; Wongkham, S.; Wongkham, C.; Somintara, O.; Sangkhamanon, S.; et al. Apoptosis-Inducing Factor, Mitochondrion-Associated 3 (AIFM3) Protein Level in the Sera as a Prognostic Marker of Cholangiocarcinoma Patients. Biomolecules 2020, 10, 1021. https://doi.org/10.3390/biom10071021
Chua-on D, Proungvitaya T, Tummanatsakun D, Techasen A, Limpaiboon T, Roytrakul S, Wongkham S, Wongkham C, Somintara O, Sangkhamanon S, et al. Apoptosis-Inducing Factor, Mitochondrion-Associated 3 (AIFM3) Protein Level in the Sera as a Prognostic Marker of Cholangiocarcinoma Patients. Biomolecules. 2020; 10(7):1021. https://doi.org/10.3390/biom10071021
Chicago/Turabian StyleChua-on, Daraporn, Tanakorn Proungvitaya, Doungdean Tummanatsakun, Anchalee Techasen, Temduang Limpaiboon, Sittiruk Roytrakul, Sopit Wongkham, Chaisiri Wongkham, Ongart Somintara, Sakkarn Sangkhamanon, and et al. 2020. "Apoptosis-Inducing Factor, Mitochondrion-Associated 3 (AIFM3) Protein Level in the Sera as a Prognostic Marker of Cholangiocarcinoma Patients" Biomolecules 10, no. 7: 1021. https://doi.org/10.3390/biom10071021