

Abstract
Background: Preoperative chemoradiotherapy (CRT) has been widely used to improve local control of disease and to preserve the anal sphincter in the treatment of rectal cancer. However, the response to CRT differs among individual tumors. Our purpose of this study was to identify a set of discriminating genes that can be used for characterization and prediction of response to CRT in rectal cancer. Patients and Methods: Seventeen rectal cancer patients who underwent preoperative CRT (40 Gy radiotherapy combined with S-1) were studied. Biopsy specimens were obtained from rectal cancer patients before preoperative CRT and were analyzed by focused DNA microarray (132 genes) and immunohistochemistry. Response to CRT was determined by histopathologic examination of surgically resected specimens and patients were classified as responders (grade 2 or 3) or non-responders (grade 0 or 1). Results: Of the 17 samples, 10 were classified as responders and 7 as non-responders. Seventeen genes were differentially expressed at significant levels (p<0.05) between responders and non-responders. All genes showed higher expression in responders as compared with non-responders. The list of discriminating genes included matrix metalloproteinase- (MMP), apoptosis- (nuclear factor kappa light polypeptide gene enhancer in B-cells 2 (NFKB2), transforming growth factor beta 1 (TGFB1)), DNA repair- (topoisomerase 1 (TOP1)), and cell proliferation (integrin, beta 1 (ITGB1))-related genes. In the immunohistochemistry of MMP7, 4 responders were judged as showing overexpression of MMP7. On the other hand, none of the non-responders were judged as showing overexpression of MMP7. Conclusion: Gene expression patterns of diagnostic biopsies can predict pathological response to preoperative CRT with S-1 in rectal cancer.
- Tailored therapy
- focused DNA microarray
- S-1
- chemoradiotherapy
- rectal cancer
- gene expression profiling
Locoregional recurrence after resection of rectal cancer is difficult to treat and is associated with severe debilitating symptoms. The prognosis after a local recurrence is poor, with a median survival of 12-18 months (1). Preoperative chemoradiotherapy (CRT) has been widely used as a major treatment modality for locally advanced rectal cancer. Clinical trials have demonstrated that preoperative CRT significantly reduces the risk of local recurrence and toxicity compared with postoperative CRT, but with similar survival rates (2-7). Furthermore, the ability to achieve pathologic downstaging or a complete pathologic response after preoperative CRT is correlated with improved survival, decreased local recurrence, and a higher rate of sphincter-preserving surgery (8-10).
Approximately 40-60% of locally advanced rectal cancer patients treated with preoperative CRT achieve some degree of pathologic downstaging. However, response to CRT differs among individual tumors and there is no effective method of predicting which patients will respond to neoadjuvant CRT. Although responders to CRT have many benefits of CRT, non-responders may unfortunately be subject to the risk of toxicity with no apparent gain. It is therefore of the utmost importance to identify factors prior to preoperative CRT that predict whether a patient is likely to be resistant or sensitive to CRT. The ability to analyze predictive markers of CRT at the levels of RNA, DNA, and protein promises to revolutionize our understanding of the disease process, and it is hoped that the era of genomics, transcriptomics, and proteomics will herald new biomarkers of response to CRT. One strategy, using gene array technology, is to compare the relative gene expression profiles of tumors between responders and non-responders to CRT.
In this report, to predict response to CRT with S-1 before preoperative CRT, we examined the gene expression patterns of diagnostic biopsy samples by customized and focused DNA microarray developed to measure molecular markers involved in response to 5-fluorouracil (5-FU) and other anticancer drugs. The purpose of this study was to define the gene expression patterns for prediction of response to CRT with S-1 and establish tailored therapy for rectal cancer.
Patients and Methods
Patients and tissue samples. For gene expression profiling, rectal cancer samples were obtained from 20 patients approved to receive preoperative CRT from September 2005 to September 2007 at Tokushima University Hospital. The 20 independent rectal tumor samples included 17 for training and 3 for testing the outcome prediction model, respectively. The patient characteristics and response to CRT are summarized in Table I. We obtained study approval from the Ethics Committee at Tokushima University Hospital and each patient gave written informed consent for samples to be used. Biopsy specimens were prospectively collected during colonoscopic examination from rectal cancer before starting preoperative CRT. Parallel tumor specimens were formalin fixed and paraffin embedded for histologic examination and further specimens were used for RNA extraction. Samples were used for RNA extraction when parallel specimens contained at least 70% tumor cells. Samples were snap-frozen immediately in liquid nitrogen and stored at –80°C until RNA extraction was carried out.
All patients received CRT with a total dose of 4,000 cGy of pelvic irradiation; CRT was administered five times weekly, with a daily fraction of 200 cGy, utilizing a four-field technique. Radiation was delivered concomitantly with S-1, a novel oral fluoropyrimidine inhibitor of dihydropyrimidine dehydrogenase which has a potent radiosensitizing property. S-1 was administered on days of radiation. Surgical treatment was performed 6-8 weeks after the completion of preoperative CRT.
Customized DNA microarrays. A customized DNA array (132 genes) has been developed to measure simultaneously molecular markers involved in response to 5-FU and other anticancer drugs. They consist of 30 genes related to pyrimidine/purine/folate metabolism (thymidylate synthase, dihydropyrimidine dehydrogenase, etc.), 19 genes related to DNA repair (DNA ligase I, uracil-DNA glycosylase, etc.), 8 genes related to drug resistance (P-glycoprotein, topoisomerase I, etc.), 7 genes related to apoptosis (P53, etc.), 24 genes related to proliferation (vascular endothelial growth factor, histone deacetylase 1, etc.), 20 genes related to cell cycle (E2F1, cyclin A1, etc.), 21 other genes of DNA methylation, cell adhesion and collagen catabolism (DNA (cytosine-5)-methyltransferase 1, CD34, matrix metalloproteinase 1, etc.) and 3 housekeeping genes (glyceraldehyde-3-phosphate dehydrogenase, beta-actin, 40S ribosomal protein S9). Target DNAs made from the 132 genes were immobilized on a glass plate. Each target DNA (200-600 bp) was designed based on sequence homology analysis to minimize cross-hybridization with other genes, and was practically tested by Northern blot. It was possible to relative determine all genes in a single assay. The basic technology of the customized DNA array is almost the same as that of a Stanford-type cDNA microarray.
Frozen tumor tissues were suspended in RLT Buffer (Qiagen, Hilden, Germany) and homogenized using an MM300 Mixer Mill (F. Kurt Retsch GmbH & Co., Haan, Germany). RNA extraction was performed using an RNeasy mini kit (Qiagen). Total RNA quality was judged from the relative intensities of the 28S and 18S ribosomal RNA bands after agarose gel electrophoresis. Purified total RNA (20 μg) was incubated at 70°C for 5 min and cooled on ice. It was reverse-transcribed with a mixture of specific primers and 200 units of PowerScript reverse transcriptase, and incubated at 42°C for 1.5 h. The cDNA was labeled using Cy5 (Cy5 monofunctional reactive dye, Cat. No. PA25001, GE Healthcare–Amersham Biosciences, Piscataway, NJ, USA), and purified by a Nucleo Spin Extract kit (Macherey-Nagel GmbH & Co. KG, Dueren, Germany). Labeled cDNA was hybridized in 6× SSC, 0.2% SDS, 0.01 mg/ml Human Cot-1 DNA and 5× Denhalt's solution for 16 h at 60°C for spotted cDNA arrays. The slides were washed in 2× SSC at room temperature, then 2× SSC with 0.2% SDS at 55-65°C twice, and finally 0.05× SSC at room temperature and scanned using an FLA-8000 Scanner (FujiFilm, Tokyo, Japan). Data was analyzed using an Array Gauge (FujiFilm).
Patient characteristics and response to CRT.
Immunohistochemistry. Immunohistochemical staining was performed on 5-μm thick sections obtained from formalin-fixed and paraffin-embedded tissue blocks of biopsy specimens from rectal cancer patients before starting preoperative CRT. Immunostaining was carried out after heat-based antigen retrieval (20 min, 95°C water bath, citrate buffer [pH 6]) using mouse monoclonal antibody against matrix metalloproteinase-7 (MMP7) (Daiichi Fine Chemical, Toyama, Japan; dilution, 1:50). Automated immunohistochemistry was performed using a Dako Autostainer Plus System (DakoCytomation, Carpinteria, CA, USA) with antimouse IgG EnVision Plus detection kit (DakoCytomation) for secondary and tertiary immunoreactions. Reaction products were developed with diaminobenzidine (DAB), according to standard protocols. Sections were considered to demonstrate MMP7 overexpression if more than 50% of the tumor cells were positively stained. Negative control sections with the omission of the primary antibody were included in each run.
Data analysis. To identify genes that were differentially expressed between the two groups, the data sets were assigned to either responders or non-responders. Response to CRT was evaluated by histopathologic examination and DNA microarray was analyzed. Histopathologic examination of surgically resected specimens was based on a semiquantitative classification system as described in detail previously (11). Tumors were classified as ”responder” when assigned to the regression grade 2 or 3, and “non-responder” when grade 0 or 1.
Genes differentially expressed between responders and non-responders.
{kind=link}
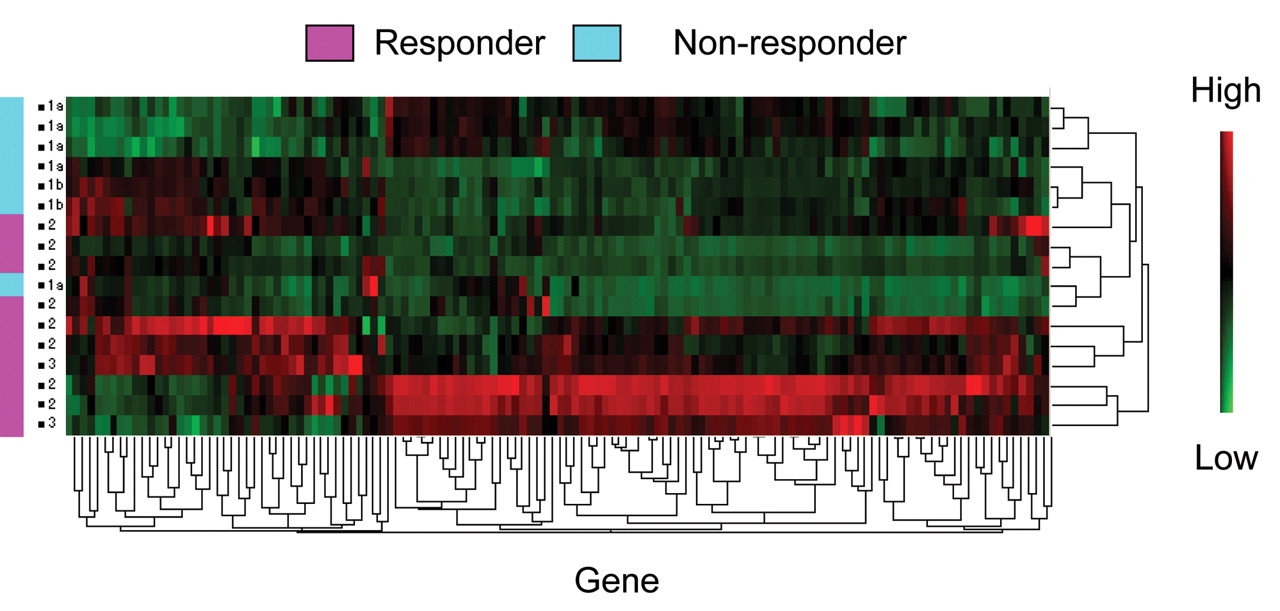
A hierarchical cluster analysis of 132 genes. Red, Overexpression; green, underexpression. Responders and non-responders were clustered into two distinct groups except for four responder cases.
Samples from 20 patients were divided into a training set (17 samples) and a testing set (3 samples). Only training samples were used in the DNA microarray analysis to evaluate gene expression. The expression patterns were compared and fold-change value calculated to identify gene markers that can best discriminate between responders and non-responders. Two-dimensional hierarchical clustering was then applied to the log-transformed data with average-linkage clustering with standard correlation as the similarity metric for the discriminating genes that were identified as being differentially expressed between responders and non-responders. Next, using immunohistochemistry in a training set, we evaluated a candidate gene, MMP7, detected by DNA microarray analysis as being the most highly overexpressed. Additionally, in a testing set, the gene expression patterns of diagnostic biopsy samples were evaluated by focused DNA microarray before preoperative CRT regarding to the histopathologic examination of surgical specimens.
Statistics. Quantitative data were given as median (range). All statistical analysis was performed using statistical software (JMP 8.0.1., SAS, Cary, NC, USA). A comparison of immunohisto-chemistry data was performed using Fisher's exact test, as appropriate. The expression patterns in the DNA microarray were compared using unpaired t-tests (with Welch's correction for unequal variances). All statistical tests performed were two-sided and declared at the 5% significance level.
Validation of the gene expression patterns by microarrays.
Results
Gene expression patterns by microarray in responders and non-responders. Gene expression profiling was established using customized and focused DNA microarray in training samples. There was no significant difference between the training set and the testing set in clinicopathologic factors such as gender, age, histopathologic classification, preoperative tumor stage, response to CRT, and so on. The patient characteristics and response to CRT are summarized in Table I. Among the 17 training samples, 10 were classified as responders and 7 as non-responders, according to the histopathologic examination of surgical specimens. Regarding histopathologic examination of surgically resected specimens, 17 genes were identified that were significantly (p<0.05) differentially expressed between responders and non-responders (Table II). All genes showed higher expression in responders as compared with non-responders. The 17 genes were matrix metalloproteinase 7 (MMP7), MMP14, MMP9, MMP1, integrin, alpha 2 (ITGA2), nuclear factor kappa light polypeptide gene enhancer in B-cells 2 (NFKB2), cathepsin B (CTSB), integrin, beta 1 (ITGB1), MMP16, plasminogen activator, urokinase receptor (PLAUR), ribonucleotide reductase M1 (RRM1), DNA (cytosine-5)-methyltransferase 1(DNMT1), uridine phosphorylase (UP), topoisomerase 1 (TOP1), transforming growth factor, beta 1 (TGFB1), nucleoside diphosphate kinase A (NDKA), and nucleoside diphosphate kinase B (NDKB). Results of a hierarchical cluster analysis of the 132 genes are presented in Figure 1. Responders and non-responders were clustered into two distinct groups except for four responder cases.
Immunohistochemistry of MMP7. MMP7, as a candidate gene, showed the highest fold-change in responders as compared with non-responders in histopathologic examination, and was chosen for validation of DNA microarray data by immunohistochemistry. MMP7 was evaluated by using immunohistochemistry examination in a training set. Four cases out of the responders (n=10) were judged as showing overexpression of MMP7. On the other hand, none of the non-responders (n=7) were judged as showing overexpression of MMP7. There was a tendency for there being a difference in expression of MMP7 between responders and non-responders.
Validation of the gene expression patterns by microarrays. Gene expression profiling (17 genes) was validated using customized and focused DNA microarray in testing samples. Among the three testing samples, two were classified as responders and one as non-responders according to the histopathologic examination of surgical specimens (Table I). One case of the responders showed overexpression of 5 out of 17 genes. Another case in the responders showed overexpression of 4 out of 17 genes. These overexpressed genes included MMP7 and TGFB1. On the other hand, the non-responder case showed no overexpression of any of the genes studied (Table III).
Discussion
Although gene expression patterns have been applied to the outcome prediction of multiple types of cancer, there are few studies to date that have reported the application of DNA array to predict response to CRT using preoperative biopsy tissue samples for rectal cancer. We defined the gene expression patterns for prediction of response to CRT by customized and focused DNA microarray and validated a candidate gene (MMP7) by immunohistochemistry.
Regarding DNA microarray, two studies have incorporated microarray analyses to assess gene expression profiles to predict CRT outcome in rectal cancer. In a study by Ghadimi et al. (12), 23 pretreatment tumor biopsies were evaluated by cDNA microarrays. The analysis revealed 54 to be genes differentially expressed between responders and non-responders, on the basis of downstaging (p<0.001). Using the leave-one-out cross-validation (LOOCV) method, 19 out of 23 patients had their response accurately predicted by their gene expression profiles (p=0.02). Using this method, 7 out of 9 responders and 12 out of 14 non-responders were correctly identified. In a validation set comprising 7 different tumor samples, 39 out of the original 54 genes identified from the training set were found to be differentially expressed. In the validation set, the gene expression profile was able to accurately predict response in six out of seven tumors.
Additionally, Rimkus et al. (13) evaluated pretreatment biopsies of 43 rectal cancer patients treated with neoadjuvant CRT. The microarray analysis revealed 42 genes to be differentially expressed among responders and non-responders, according to tumor regression grading. These 42 genes were identified from the 50 probe sets with the lowest p-values according to the Welch test. Using the LOOCV method, 10 out of 14 responders were correctly predicted, whereas 25 out of 29 non-responders were correctly predicted. In addition, 38 out of the 43 patients were selected randomly for a training set to develop a response classifier. This response classifier was used to predict response status in a small validation set consisting of five patients. The classifier predicted response in the validation-set patients with similar accuracy to the LOOCV method.
Both previous studies (12, 13) reported the ability to accurately determine responders and non-responders on the basis of microarray-determined gene expression profiles. However, between the 54 genes differentially expressed in the Ghadimi study and the 43 genes differentially expressed in the Rimkus study, there was no concordance, not even for a single gene. Furthermore, including our study, there was no concordance for any gene among the three studies. These studies, with a small number of patients, may not have sufficient power to validate the use of microarray-determined gene expression profiles to predict response to neoadjuvant CRT in rectal cancer. Kuremsky et al. (14), in a critical review of DNA microarray analysis, reported that although gene array expression data generate interesting results that may lead to the further exploration of candidate genes, the complexity and magnitude makes the results difficult to interpret.
Regarding the prediction of response to CRT using immunohistochemistry, Kuremsky et al. (14) reported that the six most commonly researched biomarkers evaluated were p53, epidermal growth factor receptor (EGFR), thymidylate synthase (TYMS), Ki-67, p21, and BCL-2/BAX. There is currently not enough evidence to suggest the clinical application of any biomarker to predict outcome in rectal cancer. We evaluated immunohistochemistry of MMP7, as a candidate gene, which showed the highest fold change in responders as compared with non-responders in histopathologic examination. Although MMP7 expression has not been previously described in rectal cancer as a biomarker to predict response of CRT, MMP7 appears to be a candidate biomarker, requiring future investigation.
The expression of MMP7 in several types of cancer has been confirmed (15-17). The direct interaction of individual MMPs, particularly MMP7, with the genes and proteins involved in colorectal cancer development has been shown (18, 19). Specifically, the MMP7 protein and its mRNA are also consistently expressed in liver metastases of colon cancer (18, 20). Our data suggest that preoperative CRT may be able to improve the prognosis of advanced rectal cancer patients with overexpression of MMP7.
Our validation of the gene expression patterns by microarrays revealed TGFB1, a gene related to apoptosis. TGFB1 is a tumor suppressor gene. Barcellos-Hoff et al. showed in mice that activation of Tgf-b is an early and sensitive response to irradiation (21). In addition to acting as a tumor suppressor, TGFB has also been shown to have a pro-tumorigenic effect (22). Induction of Ras was shown to decrease the growth-inhibitory response to TGFB (23). There are reports showing that K-ras signaling may play a role in the conversion of TGFB from a tumor suppressor to a tumor promoter (24).
The present study defined the gene expression patterns for prediction of response to CRT with S-1 by customized and focused DNA microarray and validated its ability by immunohistochemistry and microarray using preoperative biopsy tissue samples in rectal cancer. Although the key weaknesses of this study are small sample, retrospective native and unsatisfactory analysis of validation, we evaluated gene expression patterns for prediction of response to CRT with S-1 by customized and focused DNA microarray. A multicenter randomized study for prediction of response to CRT (S-1 vs. UFT) by customized and focused DNA microarray is currently in progress. It will be necessary to confirm the usefulness of gene expression patterns for the prediction of response to CRT by larger prospective studies.
Conclusion
Gene expression patterns of diagnostic biopsies can predict pathological response to CRT with S-1 in rectal cancer.
Author Disclosures
Mitsuo Shimada received research funding from TAIHO Pharmaceutical. Co. Ltd. Drs. Masanori Nishioka, Nobuhiro Kurita, Takashi Iwata, Shinya Morimoto, Kozo Yoshikawa, Jun Higashijima and Tomohiko Miyatani have no conflicts of interest or financial ties to disclose.
Acknowledgments
This study was partly supported by the Research Support Foundation of The University of Tokushima and TAIHO Pharmaceutical co., LTD., and the Grants-in-Aid for Scientific Research of the Japan Society for the Promotion of Science. A part of this study was presented at the Gastrointestinal Cancer Symposium, Florida, USA (Jan. 25-27, 2008).
- Received January 15, 2011.
- Revision received February 13, 2011.
- Accepted February 14, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved