

Abstract
Background: Despite advances in our understanding on the pathogenesis of gastric cancer (GC), patients face a poor prognosis. To improve clinical outcomes, effective approaches to diagnosis and treatment employing new diagnostic biomarkers are required to achieve early detection and predict recurrence and prognosis. Materials and Methods: Transcriptome analysis was conducted using surgically resected gastric tissues from four patients with metastatic GC. A total of 228 pairs of primary GC tissues and corresponding normal adjacent tissues were subjected to mRNA expression analysis. To validate our findings, we accessed an integrated microarray dataset and RNA sequencing data of GC cell lines. Results: We identified stimulated by retinoic acid 6 (STRA6) as a differentially overexpressed gene, which encodes a transmembrane protein that mediates the cellular uptake of retinol. To investigate how STRA6 contributes to the malignant phenotype of GC cells, we mined public datasets and found the mRNA encoding retinol binding protein 1 (RBP1), which is associated with retinoid metabolism, was co-expressed with STRA6. Furthermore, STRA6 mRNA levels were significantly higher in GC tissues compared to the corresponding noncancerous adjacent tissues of 228 surgically resected gastric tissue samples. Moreover, patients with high levels of STRA6 mRNA experienced significantly shorter disease-free survival and overall survival. Multivariate analysis revealed that high levels of STRA6 served as a significant risk factor. Conclusion: Patients with high levels of STRA6 mRNA experienced significantly worse clinical outcomes, indicating that STRA6 may serve as a diagnostic and prognostic biomarker of GC.
- Gastric cancer
- STRA6
- recurrence
- prognosis
- biomarker
Gastric cancer (GC) is characterized by diverse genomic alterations. The molecular classification of GC described in The Cancer Genome Atlas as well as emerging molecular targeted and immune checkpoint therapy indicate the possibility for developing a genomics-based personalized strategy for treating patients with advanced disease (1-3). Despite advances in our understanding of the pathogenesis of GC, prognosis is poor, mainly due to early asymptomatic lymph node metastasis, leading to incurable hematogenous recurrence (4, 5). Further, peritoneal metastasis is difficult to detect when GC recurs (6-8). Therefore, effective diagnostic biomarkers for early detection and prediction of recurrence, as well as for disease prognosis are required (3, 9, 10).
For this purpose, we herein conducted a transcriptome analysis to identify genes expressed in association with the aggressive phenotype of GC. We focused on stimulated by retinoic acid 6 (STRA6), which was differentially overexpressed in primary GC tissue of patients with metastatic disease, because retinoid metabolism is considered to be involved in carcinogenesis. Previous studies have shown that STRA6 expression is up-regulated in colorectal cancer and ovarian cancer (11, 12) although whether it is associated with GC is unknown. We, therefore, aimed to evaluate the clinical significance of STRA6 expression in GC and explored its potential utility for diagnosis and predicting prognosis.
Materials and Methods
Participants informed consent. This study conformed to the ethical guidelines of the World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects and was approved by the Institutional Review Board of Nagoya University, Japan (Study Approval Number 2014-0043). Written informed consent for use of clinical samples and data was obtained from all patients.
Transcriptome analysis. Surgically resected gastric tissues from four patients with metastatic GC were subjected to transcriptome analysis. Global expression profiling was conducted using the HiSeq platform (Illumina, San Diego, CA, USA) to compare the expression levels of 57,749 unique mRNAs expressed in primary GC tissues with those of the corresponding noncancerous adjacent gastric mucosa.
Reverse-transcription polymerase chain reaction (RT-PCR) analysis. The levels of STRA6 mRNA in clinical samples were determined in triplicate using RT-PCR analysis as previously described (13, 14). The STRA6 primers were as follows: forward 5’-CTATGGCAGCTGGTACATCG-3’ and reverse 5’-TACAGGCCGGGTGGTATG-3’. The level of the mRNA encoding glyceraldehyde-3-phosphate dehydrogenase (GAPDH) served as a standard for comparisons. Triplicate samples were subjected to quantitative real-time RT-PCR (qRT-PCR). The expression level of each sample is presented as the amount of the STRA6 amplicon divided by that of GAPDH.
Clinical samples. From 2001 through 2017, 228 pairs of primary GC tissues and corresponding normal adjacent tissues were collected from surgical specimens of patients who underwent curative gastric resection for GC without neoadjuvant therapy at the Department of gastroenterological surgery, Nagoya University Hospital. Tissue samples were immediately frozen in liquid nitrogen after collection and stored at −80°C. Specimens were histologically classified using the Union for International Cancer Control (UICC) classification, seventh edition. Patients were pathologically diagnosed with stages I–III GC, and relevant clinicopathological parameters were acquired from medical records. Since 2006, adjuvant chemotherapy using S-1 (an oral fluorinated pyrimidine) has been administered to all patients with UICC stage II-III gastric cancer, unless contraindicated by the patient's condition (15-17).
Bioinformatic analysis. To validate our experimental data, we accessed an integrated microarray dataset comprising the data of 1,065 patients from three major cancer Research Centers (Berlin, Bethesda, and Melbourne datasets; http://kmplot.com/analysis/). RNA sequencing data of 37 GC cell lines were obtained from the Cancer Cell Line Encyclopedia (https://portals.broadinstitute.org/ccle). We used these datasets to determine the prognostic significance of STRA6 mRNA expression and identify genes that were coordinately expressed with STRA6.
Statistical analysis. Qualitative variables were compared using the χ2 test, and quantitative variables were compared using the Mann–Whitney test. Disease-free (DFS) and overall survival (OS) rates were calculated using the Kaplan–Meier method, and the difference in survival was analyzed using the log-rank test. We performed multivariate regression analysis with the Cox proportional hazards model to detect prognostic factors, and variables with p<0.05 were entered into the final model. To adjust for multiple testing, we employed a false discovery rate (FDR) approach and computed the q-value. Statistical analysis was performed using the JMP 14 software (SAS Institute, Cary, NC, USA) and R version 3.4.1 (Vienna, Austria. URL: http://www.R-project.org/). p<0.05 indicates a statistically significant difference.
Results
Identification of STRA6 as a putative driver of GC. We analyzed the transcriptomes of primary gastric cancer tissues of patients with metastatic GC to identify putative driver genes associated with an aggressive phenotype. We found that 31 genes were differentially expressed at higher levels in GC tissues compared to those of adjacent normal tissues (Table I). We focused on STRA6 because of the association of retinol metabolites with the progression of GC and, to our knowledge, the absence data for STRA6 expression in GC.
Correlation analysis of STRA6 expression using an external dataset. To evaluate the role of STRA6 in cancer progression, we performed correlation analysis using the CCLE dataset to identify genes differentially expressed in association with STRA6. The top five mRNAs with the highest correlation, according to the adjusted false discovery rate (FDR), are listed in Table II. We focused on the gene encoding retinol-binding protein 1 (RBP1), which serves as a carrier protein involved in the transport of retinol. These data suggest that STRA6 and RBP1, which are related to retinol metabolism, may activate a common signaling pathway leading to gastric carcinogenesis.
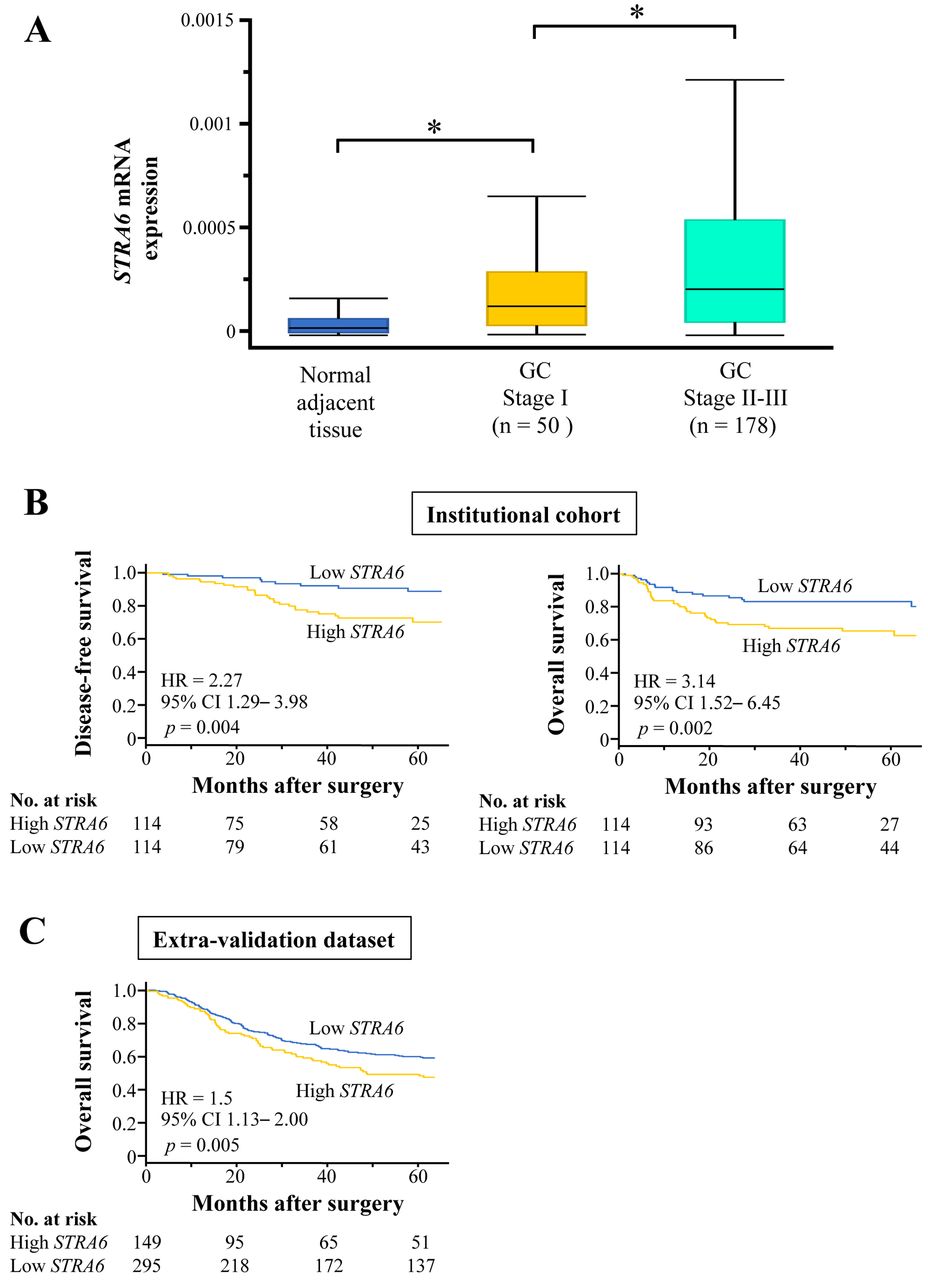
Clinical significance of STRA6 expression in surgically resected gastric tissue. The median age of the 228 patients was 67 years (range=26-96 years), and the male:female ratio was 164:64. According to the UICC staging system (seventh edition), 50, 71, and 107 patients exhibited the characteristics of GC pathological stages I, II, and III, respectively. STRA6 mRNA levels were significantly higher in GC tissues compared to those of the corresponding noncancerous adjacent tissues. Moreover, higher levels of STRA6 mRNA were expressed during the late stages of GC (Figure 1A). Patients were assigned according to their median STRA6 mRNA level in GC tissues as follows: high-STRA6 expression group, n=114; low-STRA6 expression group, n =114. The characteristics of two groups are presented in Table III. Most key clinical variables, except the UICC stage, were equally distributed between groups. Higher levels of STRA6 mRNA were significantly associated with shorter DFS and OS [hazard ratio (HR)=2.27, 95% confidence interval (CI)=1.29-3.98, p=0.004; HR=3.14, 95% CI=1.52-6.45, p=0.002, respectively] (Figure 1B). Multivariate analysis revealed that high levels of STRA6 mRNA had the highest HR among candidate risk factors (HR=2.42, 95% CI=1.14–5.13, p=0.021) (Table IV).
To further investigate the clinical significance of STRA6, we assessed survival rates using the prognostic data acquired from external validation datasets. A consistent result was observed in the extra-validation cohort of 444 patients with stage I-III GC (Figure 1C). Furthermore, the frequencies of initial recurrence sites, particularly lymph node metastasis, were significantly higher in the high-STRA6 expression group (Figure 2).
List of candidate genes expressed at increased levels in primary tumor tissues of patients with metastatic gastric cancer.
List of genes strongly correlated with STRA6 mRNA expression level in GC cell lines.
Discussion
Herein we identified STRA6 as a candidate causative gene of GC that was associated with highly malignant tumor cell phenotypes. Moreover, patients with relatively higher levels of STRA6 mRNA in GC tissues vs. controls experienced significantly shorter OS. To the best of our knowledge, the present report is the first to implicate STRA6 as a putative oncogene in GC.

STRA6 mRNA expression in clinical samples and survival analysis. (A) Comparison of STRA6 mRNA levels in normal adjacent tissues and GC tissues according to UICC stage,. *p<0.05. (B) Kaplan–Meier analysis of disease-free survival (DFS) and overall survival (OS) in the institutional cohort. The analyses included 228 patients who underwent curative gastrectomy for stages I-III GC. (C) Kaplan–Meier analysis of OS in the external validation cohort. OS analysis included 444 patients who underwent curative gastrectomy for stages I-III GC.
Association between the expression of STRA6 mRNA and clinicopathological parameters of 228 patients with stage I-III gastric cancer.
STRA6 serves as a cytokine signaling receptor, in addition to its role as a retinol transporter, and activates a JAK2/STAT3 cascade through retinol uptake and intracellular metabolism, leading to induction of multiple pro-oncogenic STAT target genes (18-20). Karunanithi et al. (12) showed that this STRA6/JAK2/STAT3 signaling cascade is one putative mechanism underlying the tumorigenesis of colon cancer. To investigate the interactions between STRA6 and other proteins that contribute to the malignant phenotype of GC cells, we investigated STRA6 expression using the CCLE datasets, and found that the expression of RBP1 significantly associated with that of STRA6 in GC cell lines. RBP1, which is the intracellular acceptor of retinol, triggers phosphorylation of a tyrosine residue in the cytosolic domain of STRA6, resulting in recruitment and activation of the JAK2 and, in a cell-dependent manner, the transcription factor STAT3 (18, 19). Consequently, RBP1 contributes to activation of the STRA6/JAK2/STAT3 signaling cascade, and triggers inflammation, proliferation, invasion, and angiogenesis. These findings further support the conclusion that STRA6 may participate in GC progression through the JAK2/STAT3 signaling cascade.
We next evaluated the association of STRA6 mRNA levels in GC tissues with patient clinical characteristics. Most clinical variables were equally distributed between the two STRA6-expression groups, except UICC stage. We found that the levels of STRA6 mRNA in GC tissues were significantly higher compared to those of the paired noncancerous tissues. Moreover, the levels of STRA6 mRNA were higher in the cancerous tissues of patients with the later stages of disease. These findings support the conclusion that elevated STRA6 expression may contribute to the initiation and progression of GC.
We observed significant differences between OS and DFS between the two STRA6 expression groups, and patients in the high STRA6 expression group experienced worse outcomes. These clinical findings are consistent with the OS of patients in the external validation dataset. Moreover, multivariate analysis revealed that high levels of STRA6 mRNA served as an independent risk factor of shorter OS. Further, higher levels of STRA6 predicted a higher incidence of recurrence, particularly lymph node metastasis. Considering that the number of patients with metastatic lymph nodes was larger (although the difference was not statistically different), the finding of a higher incidence of lymph node recurrence in the high-STRA6 group was unsurprising. Together, these results support the conclusion that STRA6 mRNA levels will serve as a biomarker for early detection as well as prediction of prognosis and detection of recurrence of GC
Carcinoembryonic antigen and carbohydrate antigen 19-9 are widely employed as biomarkers of GC, (21, 22) although our multivariate analysis revealed that elevated levels of these biomarkers were not significantly associated with patient survival. Moreover, the present study indicates that the assessment of STRA6 mRNA levels in surgically resected GC tissue, or biopsy specimens obtained from preoperative endoscopic investigations, may provide prognostic information about patients with GC. We, therefore, recommend that patients with high levels of STRA6 mRNA should be considered as candidates for undergoing enhanced perioperative chemotherapy.

{kind=link}
{kind=link}
Frequencies of initial recurrence after curative gastrectomy in patients according to STRA6 mRNA levels. *p<0.05.
Prognostic factors for overall survival of patients with stage I-III gastric cancer (n=228).
There are several limitations to the present study. First, we analyzed data acquired from a small number of patients treated at a single Institution. However, we found that our analysis of an external validation dataset was consistent with that of our patients. Further, the cut-off value of STRA6 levels and the sensitivity and specificity of detection require further optimization. Second, information about chemotherapy was unavailable, because the study's subjects were acquired over a long period during which the chemotherapeutic regimen was progressively updated. It is important to note that neoadjuvant chemotherapy is not a standard treatment for GC in Japan. Third, direct functional analyses of STRA6 were not conducted herein. Molecular genetics techniques such as RNA interference, transgenic expression of STRA6, and CRISPR/Cas9 mutagenesis will likely lead to a better understanding of the underlying mechanism of the effects of STRA6 on the pathobiology of GC. Our study provides compelling evidence that the JAK2/STAT3 cascade contributes to STRA6-mediated tumor progression. Nevertheless, further research is required to decipher the signal transduction pathways that mediate the putative oncogenic effects of STRA6 on gastric epithelial cells.
In conclusion, patients with high levels of STRA6 mRNA experienced significantly worse clinical outcomes, indicating that STRA6 may serve as diagnostic and prognostic biomarker of GC.
Footnotes
Authors' Contributions
SN and MK conceived the study concept and design, analysed data and wrote the manuscript. MK, DS, MK and YK contributed to data acquisition and interpretation. KO contributed to statistical analysis. CT, NH, MH, SY, GN and YK revised the draft. All Authors have read and approved the final version of the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors have no conflicts of interest with regard to the present study.
- Received April 15, 2020.
- Revision received May 20, 2020.
- Accepted May 29, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved