

Abstract
Background/Aim: Dedifferentiated liposarcoma (DDLPS) is recalcitrant type of sarcoma. DDLPS has a low survival rate with high recurrence and metastasis. In the present study, we evaluated the efficacy of several drugs against doxorubicin-resistant DDLPS in a patient-derived orthotopic xenograft (PDOX) model for precision oncology. To establish the PDOX model, a tumor from a patient who had recurrent high-grade DDLPS from the retroperitoneum was previously grown orthotopically in the retroperitoneum of nude mice. Materials and Methods: We randomized DDLPS PDOX models into 8 treatment groups when tumor volume became approximately 100 mm3: control, no treatment; G2, doxorubicin (DOX); G3, pazopanib (PAZ); G4, gemcitabine (GEM) combined with docetaxel (DOC); G5, trabectedin (YON); G6, temozolomide (TEM); G7, palbociclib (PAL); G8, eribulin (ERB). Tumor length and width were measured both at the beginning and at the end of treatment. Results: At the end of treatment (day 14), all treatments significantly inhibited DDLPS PDOX tumor growth compared to the untreated control, except DOX. ERB was significantly more effective and regressed tumor volume compared to other treatments on day 14 after initiation of treatment. No significant differences were found in the relative body weight on day 14 compared to day 0 in any group. Conclusion: The clinical potential of ERB against DDLPS is herein presented in a PDOX model.
- Patient-derived orthotopic xenograft
- PDOX
- eribulin
- regression
- doxorubicin resistance
- dedifferentiated liposarcoma
Liposarcoma is a soft tissue sarcoma (STS). Among STS, dedifferentiated liposarcoma (DDLPS) has the lowest survival rate (1) with high recurrence and metastasis rates even after treatment with first-line therapies (2, 3). Novel more effective therapies are needed. We have previously established a patient-derived orthotopic xenograft (PDOX) nude-mouse model for all major cancers (4-15) including DDLPS (16).
Pazopanib is a tyrosine kinase inhibitor (TKI) that blocks tumor growth and inhibits angiogenesis (17). It was highly efficacious in a Phase 3 study in patients with STS (18). Gemcitabine is a cytidine analog that is extensively used in anti-cancer therapy. Gemcitabine is easily incorporated into DNA and causes cytotoxicity by inhibiting DNA replication (19-22). Docetaxel is a cytotoxic taxane that blocks mitosis (23, 24). The combination of gemcitabine and docetaxel has shown synergism (25) both in vitro (26) and in vivo (27). Recent studies demonstrated that the combination of gemcitabine and docetaxel was highly effective in patients with STS (28-30). Trabectedin is a synthetic, marine-derived alkylating agent derived from the Caribbean tunicate, Ecteinascidia turbinate (31). Trabectedin is active in patients with liposarcoma (32) and has multiple mechanisms of action (33). Temozolomide is a cytotoxic prodrug which exerts cytotoxicity mainly by methylating nucleotide bases (34). Temozolomide has shown clinical activity against high-grade brain cancer (35), melanoma (36), and pediatric rhabdomyosarcomas (37-38). A Phase II clinical trial of temozolomide on advanced STS showed an increase in progression-free survival (39).

(A) Treatment schema for the DDLPS PDOX model. (B) Efficacy of doxorubicin (DOX), pazopanib (PAZ), gemcitabine combined with docetaxel (GEM+DOC), trabectedin (YON), temozolomide (TEM), palbociclib (PAL) and eribulin (ERB) on the DDLPS PDOX model. Tumor volume was measured pre- and post-treatment. N=8 mice/group. (C) Relative tumor volume for each mouse is presented in a waterfall plot.
Cyclin-dependent kinase 4 (CDK4), is amplified in more than 90% of well-differentiated liposarcomas (WDLS)/dedifferentiated liposarcomas (DDLS) (40-42). It has been demonstrated that inhibiting the expression of CDK4 with short hairpin RNA (shRNA) inhibits growth of STS cells in vitro (43).
Eribulin, synthesized from a marine sponge Halichondria okadai (44, 45), is a non-taxane microtubule-dynamics inhibitor (46, 47). Eribulin has been approved by the Food and Drug Administration (FDA) for aggressive breast cancer patients (48). In the United States, Eribulin has been used for the treatment of patients with inoperable or metastatic liposarcoma since 2016 (49).
The present report demonstrates that a DDLPS PDOX model identified eribulin as a highly effective drug that regresses tumor volume indicating its clinical potential.
Materials and Methods
Animal care. Male athymic nu/nu nude mice (AntiCancer Inc., San Diego, CA, USA), 4-6 weeks old, were used in the present study. Mouse studies were conducted with an AntiCancer Inc. Institutional Animal Care and Use Committee (IACUC)-protocol specifically approved for this study and in accordance with the principles and procedures outlined in the National Institutes of Health (NIH) Guide for the Care and Use of Animals under Assurance Number A3873-1 (16). To minimize suffering of animals during surgery, anesthesia and analgesics were provided (16).
Patient-derived tumor. A 69-year-old male patient with DDLPS of right retroperitoneum underwent radical resection with en bloc right nephrectomy (16). Two years after surgery, local recurrence resulted (16). The patient previously underwent surgical resection at the Department of Surgery, University of California, Los Angeles, USA (UCLA) (16). Written informed consent was obtained from the patient as part of a UCLA Institutional Review Board approval protocol (IRB #10-001857) (16).
Establishment of DDLPS PDOX model. A fresh specimen of the tumor of the patient was previously obtained and transported immediately to the laboratory at AntiCancer, Inc., on wet ice (16). The detailed procedure of cutting samples into small fragments and their initial implantation subcutaneously in nude mice, to subsequently establish PDOX models and wound closure has been described in our previous publication (16).

Representative images of DDLPS PDOX models, pre- (left panels) and post- (right panels) treatment.
Treatment protocols for the DDLPS PDOX model. PDOX mouse models were randomly divided into 8 groups: G1, control no treatment; G2, doxorubicin (DOX) [3 mg/kg, intraperitoneal (i.p.) injection, weekly, for 2 weeks]; G3, pazopanib (PAZ) [100 mg/kg, p.o., daily, for 2 weeks]; G4, gemcitabine (GEM) (100 mg/kg, i.p., weekly, for 2 weeks) combined with docetaxel (DOC) (20 mg/kg, i.p., once); G5, trabectedin (YON) [0.15 mg/kg, intravenous (i.v.) injection, weekly, for 2 weeks]; G6, temozolomide (TEM) (25 mg/kg, p.o., daily, for 2 weeks); G7, palbociclib (PAL) (100 mg/kg, p.o., daily, for 2 weeks); G8, eribulin (ERB) (1.5 mg/kg, i.v., weekly, for 2 weeks) (Figure 1A). Each treatment group contained 8 mice. Tumor length and width were measured both before and after treatment. Tumor volume was calculated based on our previous studies (16). The tumor volume ratio is defined at the tumor volume at a post-treatment point relative to pre-treatment tumor volume (50).
Histological examination. Detailed protocols to fix the fresh tumor samples, embedding in paraffin, sectioning and staining were described previously (16). Hematoxylin and eosin (H&E) staining was performed according to a standard protocol (16). Histological examination was performed with a BHS system microscope and images were acquired with INFINITY ANALYZE software (Lumenera Corporation, Ottawa, Canada).
Statistical analysis. All statistical analyses were performed as previously described (50). The Student's t-test was used to determine the significant differences for continuous variables. Data are presented as mean±standard deviation (SD). A probability value p≤0.05 was considered a statistically-significant difference.
Results
Drug efficacy. At the end of treatment (Day 14), all treatments significantly inhibited DDLPS tumor growth compared to the untreated control except DOX: (DOX: p=0.61; PAZ: p=0.17; GEM+DOC: p=0.11; YON p=0.04; TEM: p=0.04; PAL: p=0.01; ERB: p=0.001). However, ERB was significantly more effective compared to DOX (p=0.001), PAZ (p=0.001), GEM+DOC (p=0.001), YON (p=0.001), TEM (p=0.001) and PAL (p=0.01). In addition, ERB significantly regressed tumor volume by the end of treatment (day 14) compared with day 0 (p=0.001) (Figures 1 and 2).

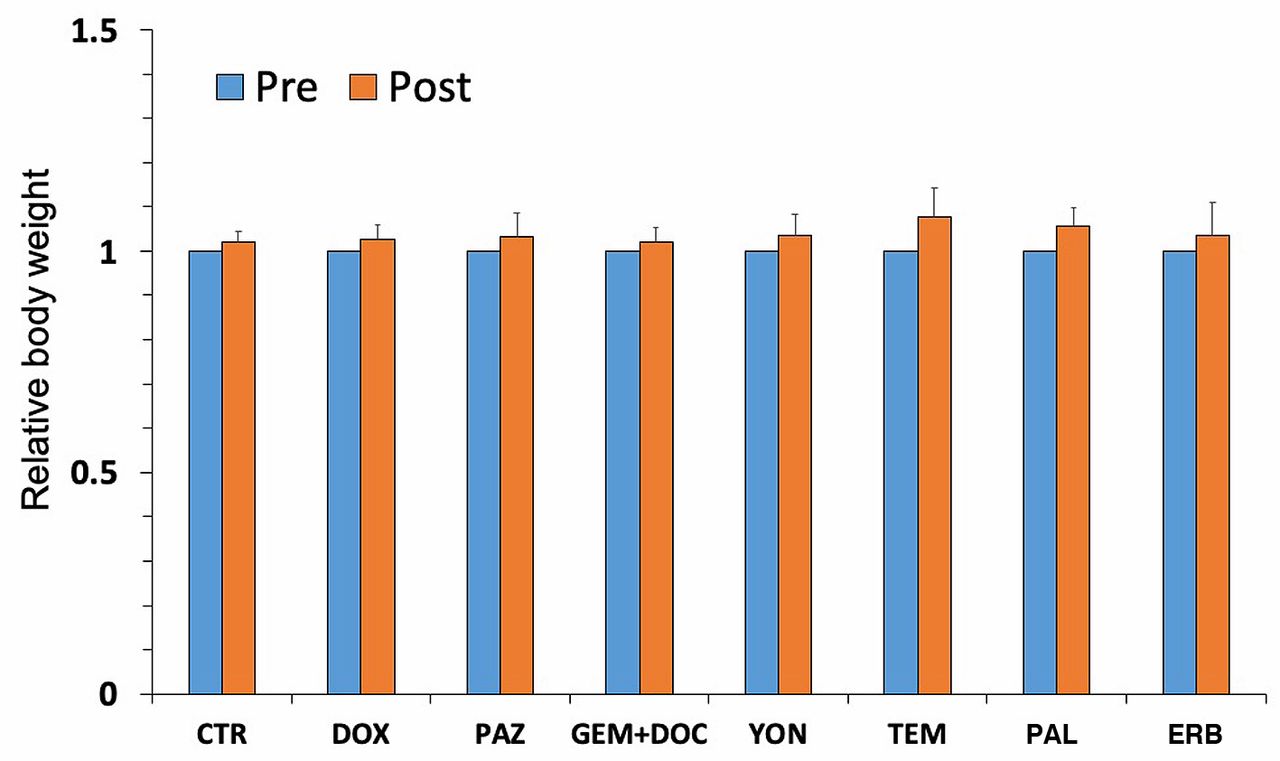
Body weight of (DOX); pazopanib (PAZ); gemcitabine combined with docetaxel (GEM+DOC); trabectedin (YON); temozolomide (TEM); palbociclib (PAL); and eribulin (ERB). Bar graph shows body weight in each group before (day 0) and after treatment (day14). N=8 mice/group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tumor histology. H&E-stained sections of the untreated PDOX tumor (A); PDOX tumor treated with doxorubicin (DOX) (B); PDOX tumor treated with pazopanib (PAZ) (C); PDOX tumor treated with gemcitabine combined with docetaxel (GEM+DOC) (D); PDOX tumor treated with trabectedin (YON) (E); PDOX tumor treated with temozolomide (TEM) (F); PDOX tumor treated with palbociclib (PAL) (G); and PDOX tumor treated with eribulin (ERB) (H). White scale bars: 50 μm.
Body weight. No significant difference was observed in the relative body weight on day 14 compared to day 0 in any treatment group (Figure 3).
Histology. High-power photomicrographs of the untreated control PDOX tumor show spindle cells with hyperchromatic and enlarged nuclei. Mitotic figures and atypical cells are present (Figure 4A). Tumors treated with DOX and PAZ had viable cells with no obvious necrosis or inflammatory changes (Figure 4B and C). Tumors treated with GEM+DOC and YON show changes in cancer-cell shapes and few necrotic cancer cells (Figure 4D and E). Tumors treated with TEM and PAL show changes in cancer-cell shapes, few necrotic cancer cells and also fibrotic areas (Figure 4F and G). In contrast, tumors treated with ERB show decreased tumor cellularity, necrotic cancer cells and tissue fibrosis (Figure 4H).
Discussion
DDLPS is a recalcitrant sarcoma with the lowest survival rate among liposarcoma. DDLPS frequently recurs or metastasizes after first therapy because no current curative options are available (1,2). Therefore, transformative, personalized and effective therapy is urgently needed for DDLPS patients.
PDOX models have provided clinically-relevant individualized mouse models of cancer since PDOX models recapitulate clinical behavior, and mimic tumor-specific drug-sensitivity (51). PDOX models of sarcoma behave very similarly to patient sarcoma in terms of recurrence after surgery (15), and metastasis (52) and invasiveness to surrounding tissue (15, 53).
Using PDOX models, multiple therapeutic agents can be tested (53-60), including targeted therapy in a preclinical model (61-66).
In the present study, ERB was found to regress the DDLPS PDOX tumor. The present study, using PDOX models, provides DDLPS patients with specific and personalized treatment options. Future studies will label the DDLPS PDOX tumors with fluorescent proteins by growing them in transgenic nude mice expressing fluorescent proteins, whereby the PDOX tumor acquires fluorescent stromal cells. Such labeled tumors will be used to detect metastasis in non-colored mice (52, 67). Thus far, all sarcoma PDOX models have correlated with drug resistance in the patient (68).
Acknowledgements
This paper is dedicated to the memory of AR Moossa, MD, Sun Lee, MD, Professor Li Jiaxi, and Masaki Kitajima, MD.
Footnotes
Authors' Contributions
Conception and design: KI and RMH. Acquisition of data: KI, KK, TK, KM and TH. Analysis and interpretation of data: KI, KK, TK, KM, TH, NY, KH, HK, SM, SRS, HT and RMH. Writing, review, and/or revision of the manuscript: KI, RMH and SRS.
This article is freely accessible online.
Conflicts of Interest
KI, KK, TK, KM, TH, NY, KH, HK, SM and RMH are or were unsalaried members of AntiCancer Inc., which uses PDOX models for contract research. There are no other competing financial interests.
- Received March 25, 2020.
- Revision received April 14, 2020.
- Accepted April 21, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved