

Abstract
Background/Aim: The ability to easily detect autoantibodies will help in the early diagnosis and treatment of certain diseases. Currently, available methods for autoantibody detection are time-consuming and cumbersome. The present study aimed to evaluate the performance of an easy-to-use antigen array developed for autoantibody detection. Materials and Methods: Plasma from 9 female donors diagnosed with ovarian cancer (test group) and 9 matched donors with no history of cancer (reference group) were screened and results were compared. Autoantibody levels ≥1.5-times the background were classified as positive. Results: A total of 29 autoantibodies were detected, out of which the autoantibody against osteoprotegerin was found to be significantly higher in the “test” group (p<0.001) while those against macrophage migration inhibitor factor, interleukin-2 and vascular endothelial growth factor were lower (p<0.05). Conclusion: The evaluated antigen array has potential as a simple method for determining the presence/absence of up to 90 disease-associated autoantibodies in a plasma specimen.
- Antigene array
- autoantibody detection
- autoimmune disease
- ovarian cancer
- plasma
The last 15 years has witnessed remarkable efforts in identifying circulating biomarkers that can be used for early detection and accurate diagnosis of diseases such as cancer. A class of protein biomarkers that has attracted significant interest are autoantibodies (1), the high-affinity and high-avidity antibodies produced by the immune system against an individual's own protein(s). Autoantibodies can be found in the blood of both healthy persons and people with disease, and their presence is usually a clear indication of existence of an immune response that may have been triggered by genetic predisposition, hormones, therapeutic drugs or an environmental component including exposure to viruses and toxic chemicals (2). It has been reported that more than 32 million Americans and an estimated 3-5% of the world population have autoimmune disorders of different severities (3-5). In addition to autoimmune, the diseases in which autoantibodies are frequently implicated, such as Type 1 diabetes, systemic lupus erythematous, scleroderma, thyroiditis, celiac disease, adrenalitis, pernicious anemia, rheumatoid arthritis, polymyositis, dermatomositis and some forms of hepatitis (2, 4), circulating autoantibodies have also been identified in multiple types of cancer.
There exist strong indications that the type and levels of autoantibodies present in the blood can serve as biomarkers for disease activity and severity. Autoantibodies would be ideal early biomarkers for disease progression because their levels could indicate the presence, nature and intensity of an individual's immune response to disease, and hence disease status, even when there are no clinical symptoms of disease (2). It is also believed that autoantibodies could be used as biomarkers to define and classify disease, e.g. in Type 1 diabetes which can be classified as an autoimmune disorder. They can also be used to predict disease, for example in organ-specific autoimmune diseases where long pre-clinical periods are common (2). Autoantibodies are very specific to the targeted protein as they are generated by mature B-cells (6). Since in autoimmune disorders the immune response is part of the disease process, it is conceivable that the type and titer of autoantibodies present in a clinical specimen can be used to predict the likelihood of clinical disease, predict the rate of progression to disease, contribute to classification of the disease, and predict the onset of disease. In fact, some autoantibodies are routinely used for diagnosis in the clinical setting, including anti-nuclear autoantibodies (ANA), anti-phospholipid autoantibodies and anti-Smith autoantibodies. Others have been used to study disease activity including autoantibodies to glutamic acid decarboxylase and protein tyrosine phosphate–like molecule IA-2 (2).
Several methods have been reported for the detection of autoantibodies in clinical and biological samples. The enzyme-linked immunosorbent assay (ELISA), fluorescence assays and high-density protein arrays are reported methods used to measure autoantibodies (4, 7-9). The ELISA and fluorescence assays are time-consuming when testing for multiple autoantibodies because they typically screen for one autoantibody at a time. Protein arrays are attractive because they provide an opportunity to simultaneously screen for hundreds to thousands of autoantibodies that may not have been previously known to be associated with the disease of interest. But the high cost of protein arrays, limited availability of necessary equipments and the level of expertise required to perform the experiment and analyze the data keeps this technology out of reach for most research scientists and laboratories. The availability of alternate, simple and inexpensive methods to screen for autoantibodies will encourage and facilitate autoantibody research, and could lead to elucidation of more autoantibodies that are relevant in disease diagnosis and treatment. We presume that a microtiter plate-based antigen array (10) would be the most simple and inexpensive method to quickly screen for the presence or absence of autoantibodies in clinical and biological samples. The positive autoantibodies can then be validated using other more specific methods.
The Autoantibody Profiling System - 90 (APS-90; ITSI Biosciences, Johnstown, PA, USA) is based on a 96-well microtiter plate format developed to allow for rapid screening of multiple autoantibodies. According to the products' literature, 90 of the wells contain probes (antigens) against proteins relevant in autoimmune diseases, 4 wells contain standards for generation of a standard curve and 2 wells contain probes for positive and negative controls. The 90 probes target autoantibodies that are reported to be present in several diseases including cancer, lupus, chronic obstructive pulmonary disease (COPD), cardiovascular disease, autism, diabetes, rheumatoid arthritis and inflammatory bowel syndrome which makes the kit ideal for discovery and verification of the presence or absence of autoantibodies. The workflow process for APS-90 is similar to that of ELISA, and the APS-90 kit includes reagents in a ready-to-use format which enhances consistency.
The central objective of the present study was to determine if APS-90 can detect autoantibodies of significance in plasma samples from two clinically distinct groups. Using plasma from female donors with and without ovarian cancer as samples, the APS-90 detected autoantibodies that occurred at significantly different levels in plasma of cancer and control groups. Ovarian carcinoma is of interest to our group because it represents the 7th leading cancer amongst women and accounts for about 3% of all female cancers (11). If validated, this could serve as a simple and inexpensive method for rapid screening of plasma for the presence or absence of multiple autoantibodies.
Materials and Methods
Human plasma samples. The plasma samples used for the study were collected from post-menopausal female donors; i) with no personal history of cancer (reference group, n=9) and ii) preoperatively from women undergoing surgery for suspected ovarian cancer whose surgical pathology later confirmed Stage IIIC ovarian cancer (test group, n=9). All samples were collected under an Institutional review board-approved protocol and stored frozen at -80°C for about 10 years prior to their use for this study. The total protein content of all samples was determined using the ToPA protein assay Kit (ITSI-Biosciences, Johnstown, PA) as previously described (12) to ensure that equal amounts of total protein were used in each assay.
Screening of plasma for autoantibodies. Undiluted plasma samples were screened with the APS-90 using the recommended protocol. Three samples in each arm were pooled so that a total of 3 APS-90 plates each were used for the pooled reference samples (R1, R2 and R3) and 3 pooled test samples (T1, T2 and T3). To screen for autoantibodies, 50 μl of plasma containing similar amounts of total protein were added to each APS-90 well and the plate was incubated on a plate shaker for 2 h at room temperature. After the incubation period, the supernatant was removed by aspiration with a pipette and discarded, the plate was washed 3 times with 300 μl of wash buffer and the detection antibody (100 μl, 1:20,000 dilution) was added to each well. The plates were then incubated at room temperature for a further 1 h and washed 4 times with 300 μl of wash buffer. Finally, 100 μl of detection solution were added to each well and the plate was incubated at room temperature for 30 min and the reaction was quenched by the addition of the ‘Stop” solution. The absorbance was measured at 405 nm with a ChroMate® microplate reader (Awareness Technologies, Palm City, FL). All optical density readings were completed within 30 min of stopping the reaction, and in each case the measurement at 655 nm was used for correction. All experiments were performed in triplicate.
Data analysis. The absorbance readings from all the wells were exported from the microplate reader as Tab Delimited files, imported into Microsoft Excel and converted to their corresponding concentrations in μg/ml using the standard curve, and the mean concentration calculated for all wells. In this study, the results were evaluated by a cut-off which was estimated by multiplying the background value by a factor of 1.5. Thus, if the sample OD405 nm is ≥1.5 of the background, the sample is classified as positive, and if it is <1.5 of the background it is classified as negative. The Student's t-test was then performed to estimate the statistical significance of the difference in specific autoantibody levels between the “test” and “reference” groups. The cut-off used for statistical significance was p<0.05. To calculate the relative abundance of each autoantibody, the mean concentration for each autoantibody detected in the “test” sample was divided with the mean concentration detected in the “reference” sample (test/reference) to obtain the ratio, thus indicating which group displayed higher autoantibody levels. Any positive autoantibody with ratio ≥1.3 was classified as higher in the test group whereas a ratio of ≤0.7 was classified as lower in the test group. The positive autoantibodies with ratios of ≥0.8 and ≤1.2 were classified as similar in levels in the test and reference groups.
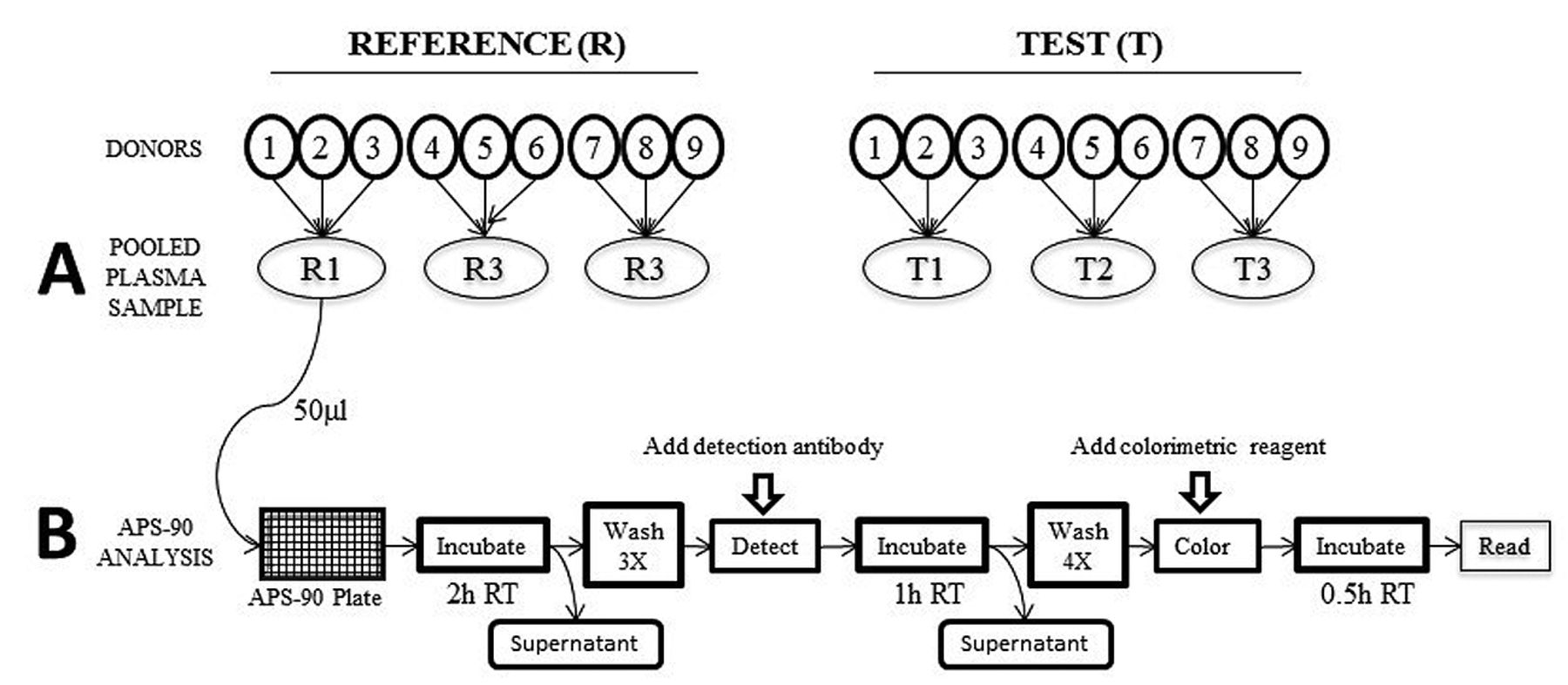
Schematic representation of the workflow for screening human plasma samples with APS-90. A: Plasma from 9 donors with no history of ovarian cancer were used as the reference group and samples from 9 donors diagnosed with ovarian cancer were used as test group. Three samples in each group were pooled to obtain 3 reference samples (R1, R2 and R3) and 3 test samples (T1, T2 and T3). B: APS-90 was used to screen 50 μl of each pooled sample. All incubations were performed at room temperature (RT) and the entire assay lasted 4h.
Results
Autoantibody detection. The primary aim of the present study was to evaluate the performance of an autoantibody profiling system in detection of autoantibodies in plasma. The APS-90 kit used contains 90 antigens that target selected autoantibodies which are reported to be present in cancer, lupus, COPD, cardiovascular disease, autism, diabetes, rheumatoid arthritis and inflammatory bowel syndrome (10). Due to our interest in ovarian carcinoma, we used plasma from donors diagnosed with ovarian cancer and those from well-matched reference donors to test the array. All the donors were post-menopausal and all the ovarian cancer patients were diagnosed with Stage IIIC ovarian cancers. The plasma samples were collected from the cancer patients prior to surgery or other therapy, which means that the obtained data are not affected by surgery or treatment. Even though the samples have been stored frozen for at least for 10 years prior to use, long-term frozen storage is not expected to significantly impact the autoantibody titers. Moreover, it is reasonable to expect that any impact due to long-term storage will affect the test and reference samples to the same extent since they were collected, stored and analyzed under the same conditions. To control for any sample variability, 3 samples within each group were pooled, as illustrated in Figure 1, which means 3 microtiter plates were used to screen 9 samples per group. The entire screening process, from the addition of 50 μl plasma to the plate and measurement of the optical density with a microtiter plate reader, lasted for about 4 h.
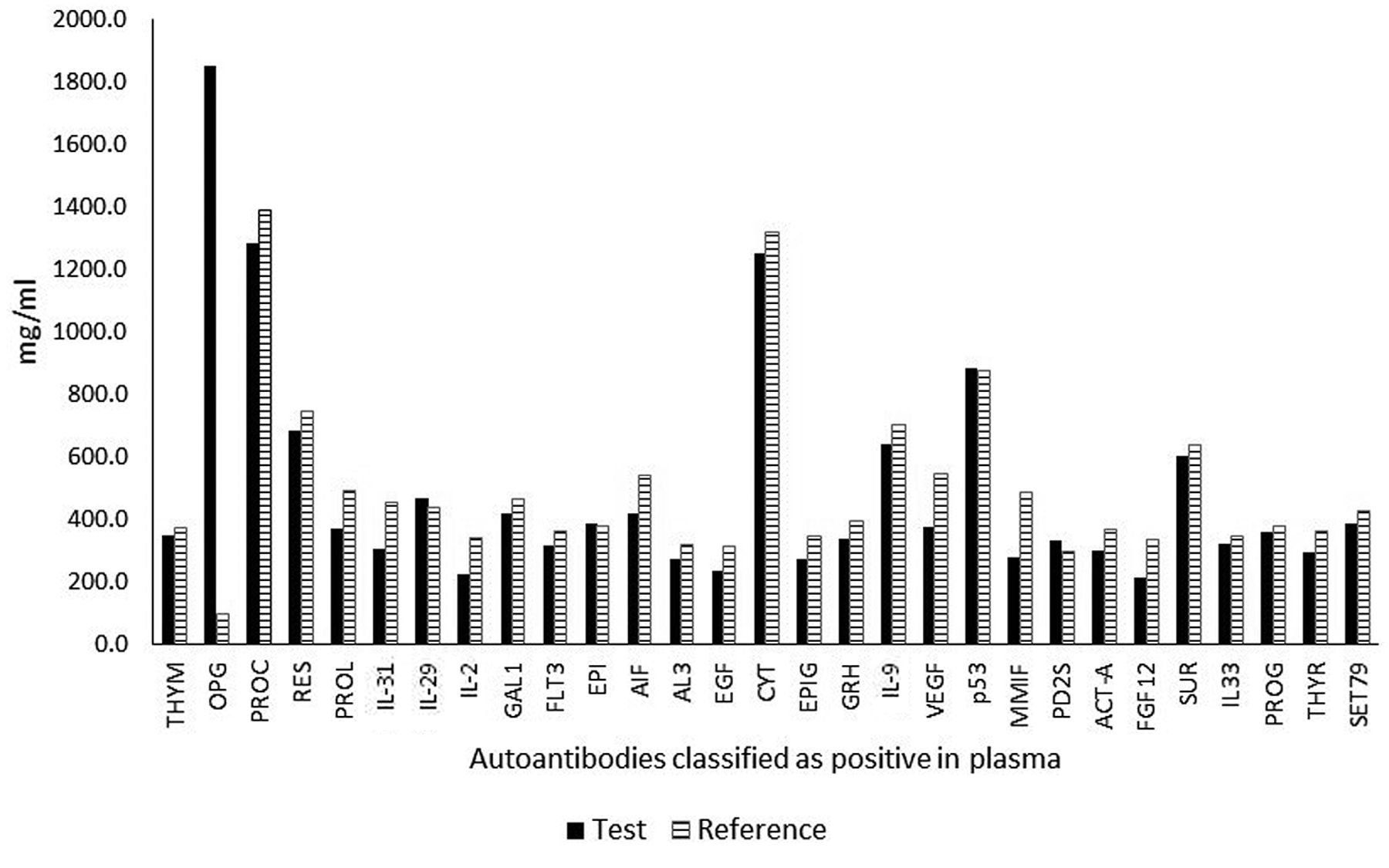
Autoantibodies detected in plasma. The optical density readings obtained were evaluated by a cut-off that was determined by multiplying the background by 1.5. Using this cut-off, a total of 29 autoantibodies were identified as elevated in the test and reference samples. Out of the 29 autoantibodies classified as positive, 4 including osteoprotegerin (OPG), macrophage migration inhibitor factor (MMIF), interleukin 2 (IL-2) and vascular endothelial growth factor (VEGF) showed statistically significant difference in levels between the “test” and “reference” groups (p<0.05; Table I).
A survey of the literature revealed that the 29 autoantibodies we classified as positive (Figure 2), have been reported in other disease conditions including cancer and autoimmune disorders (1-9). Amongst the differentially expressed autoantibodies, the autoantibody against OPG was the only autoantibody significantly elevated mainly in the “test” group, whereas the autoantibodies MMIF, IL-2 and VEGF were significantly lower in the “test” group. The autoantibodies against interleukin 29 (IL-2), epiregulin (EPI), p53 mutant (a.a 135) protein (p53) and prostaglandin D2 synthase (PD2S) were higher in the test group (Figure 2), but t-test showed no significant difference between the test and reference groups.
Discussion
Autoantibodies are detectable in the plasma of individuals with/without clinical symptoms of any disease. But it is also well-known that the presence of autoantibodies is an indication of the existence of an immune response that may have been triggered by many factors including exposure to environmental components such as viruses or toxic chemicals. For this reason, investigations involving a very limited number of samples such as those described herein are insufficient to determine whether the identified autoantibodies could truly serve as biomarkers for a specific disease. Nevertheless, the detection of autoantibodies previously reported to occur in a specific disease, in this case cancer, is an indication that the evaluated kit has potential as a cost-effective method that can be used to quickly screen a sample for the presence or absence of the autoantibodies for which the kit is designed.
{kind=link}
{kind=link}
Profile of autoantibodies against the 29 proteins detected in human plasma with APS-90. The autoantibodies detected were against the following proteins; thymic stromal lymphopoietin (THYM), osteoprotegerin (OPG), procalcitonin (PROC), resistin (RES), prolactin (PROL), interleukin-31 (IL-31), interleukin-29 (IL-29), interleukin-2 (INT2), galectin-1 (GAL1), flt3-ligand (FLT3), epiregulin (EPI), allograft inflammatory factor 1 (AIF), angiopoietin-like protein 3 (AL3), epidermal growth factor (EGF), cytotoxic t-lymphocyte associated antigen-4 (CYT), epigen (EPIG), growth hormone (GRH), interleukin-9 (IL-9), vascular endothelial growth factor (VEGF), p53 mutant (a.a 135) protein (p53), macrophage migration inhibitor factor (MMIF), prostaglandin d2 synthase (PD2S), activin-a (ACT-A), fibroblast growth factor 12 (FGF12), survivin (SUR), interleukin-33 human (IL33), progranulin (PROG), thyroglobulin human (THYR) and set7/9 histone methyltransferase (SET79). Out of these, osteoprotegerin, interleukin-2, vascular endothelial growth factor and macrophage migration inhibitor factor occurred at significantly different levels between the “test” and “reference” samples.
Autoantibodies with significant differences regarding their plasma levels between cancer and reference groups.
It is very interesting to find OPG autoantibody predominantly higher in the ovarian cancer group in this study (p<0.001). Osteoprotegerin is a cytokine receptor, and a member of the tumor necrosis factor family. It plays an important role in cancer biology, and it has been well-characterized as a negative regulator of bone re-modeling (13). It is elevated in ascites of ovarian cancer patients and is thought to protect ovarian cancer cells against apoptosis (14). Recently, it was reported that overexpression of OPG in triple-negative breast cancer promotes metastasis via modulation of protease expression and invasion (13) and the serum levels of OPG when used as one of a 6-marker panel of proteins can distinguish ovarian cancer patients from normal subjects (15, 16). If independently validated, the level of the autoantibody against osteoprotegerin could serve as a discriminating biomarker for ovarian cancer and potentially complement existing tests for ovarian cancer detection, diagnosis, prognosis or prediction.
The autoantibody against MMIF occurred at lower levels in the test group compared to the reference group (p=0.01). MMIF is involved in innate immune response, and it helps tumor cells escape from the host's natural killer cells. It has also been shown to be involved in metastasis of pancreatic cancer (17). MMIF induces the expression of other growth factors including VEGF and matrix metalloproteinases (17). Interestingly, MMIF combined with galectin has been shown to be a good prognostic marker for pancreatic cancer (18) and levels of MMIF correlate with poor prognosis of ovarian cancer (19). The finding that MMIF autoantibodies are lower in the ovarian-cancer group is noteworthy because MMIF is believed to play a suppressive role in the host anti-tumor immune response and this may have an impact on the course of the disease (19). The identification of 6 biomarkers in serum, including MMIF, that demonstrated a sensitivity of 95.3% and a specificity of 99.4% for the detection of ovarian cancer has been also reported (20).
IL-2 autoantibodies occurred at significantly lower levels in the plasma of the test group (p<0.01). This finding is very interesting because a 6-panel marker of proteins which includes interleukin-2 receptor-alpha, has been used to distinguish ovarian cancer patients from normal subjects (15). Interleukins are known to play a critical role in cancer progression and interleukin 2 is specifically necessary for production, growth and proliferation of T-cells. Cancer promotes an immunosuppressive microenvironment which enhances cancer growth and spread and some patients are now treated with administration of IL-2 (21). IL-2 is also a known poor prognostic marker for Hodgkin's lymphoma (22). It was observed that IL-2 autoantibodies were down-regulated in patients with Hodgkin's lymphoma and this finding may indicate the presence of cancer before the onset of clinical symptoms (22).
The finding that autoantibodies against VEGF occurred at significantly lower levels in the test group (p=0.03) is of interest because of the role VEGF plays in cancer. VEGF is a signaling protein produced by cells that stimulate blood vessel formation and angiogenesis. VEGF and vascular endothelial growth factor receptor (VEGFR) are the key signaling proteins that regulate proliferation and migration of endothelial cells. The levels of VEGF in the blood have been studied extensively in the context of cancer and VEGF is overexpressed in ovarian cancer (23). It is reported that VEGFRs are expressed at high levels in many types of human solid tumors, including glioma, lung, breast, renal, ovarian and gastrointestinal tract carcinomas (24). Notably, the inhibition of VEGFR has become a promising therapy for cancer and this potential has been supported by the FDA approval of bevacizumab, sorafenib, and suntinib for clinical use. Cancer treatments that target VEGF (24) have been developed because it is known that solid cancers cannot grow beyond a certain size without an adequate blood supply, and cancers that express VEGF are known to have the best metastatic potential. VEGF expression is altered in many tumors including thymic epithelial tumors (25), renal cell carcinoma (24), ovarian cancer (26) and breast cancer (27). Although it has been reported that autoantibodies against muscarinic receptors in breast cancer play a role in tumor angiogenesis (27), a search of the literature did not reveal any reported association with VEGF autoantibodies. Epidermal growth factor (EGF) autoantibodies are implicated in autoimmune diseases (23). EGF and VEGF are up-regulated in ovarian cancers and they inhibit spontaneous apoptosis. Autoantibodies against EGFR have been reported in breast cancer but do not seem to be associated with the HER2 gene amplification related to aggressive breast cancers (28). A significant difference in the serum concentration of VEGF and EGF between ovarian cancer and control groups, with 84% sensitivity and 95% specificity, has been reported (29).
Although the main objective of the study was not to identify autoantibodies that are relevant in ovarian cancer, the autoantibodies detected are noteworthy and deserve to be further investigated as candidate biomarkers for ovarian cancer. It is hoped that this article will stimulate more studies aimed at validating our finding. In a recent paper (8), the analysis of sera from ovarian cancer patients with a Nucleic Acid Protein Programmable Array (NAPPA) containing 5,177 candidate tumor antigens identified 741 autoantibodies, out of which autoantibodies against p53, PTPRA and PTGFR were found to be the top three, and achieved 23.3% sensitivity and 98.3% specificity for ovarian cancer detection, if at least two were positive. The APS–90 array used in our study contains the probe for a mutant p53 but not probes for PTPRA and PTGFR. In our study, the levels of autoantibodies against the mutant p53 protein in the test (cancer) and reference (normal), groups were above the cut-off but not significantly different. It is, however, not known if the probe used in both studies target the same mutant p53.
It is widely accepted that autoantibody markers have a number of advantages over conventional protein-oncomarkers that would make them better biomarkers for cancer detection. Such advantages include high specificity in cancer detection, high stability in blood, plasma and serum, long shelf life and minimum concentration variations because the titer is not affected by factors like diurnal variation, food/drug intake, physical activity, menstrual cycle and method of detection (30). In fact, for breast cancer it is suggested that autoantibody assays against a panel of antigens could be used as an aid to mammography for the detection and diagnosis of early primary breast cancer, especially in younger women with dense breasts at increased risk of breast cancer where mammography is known to have reduced sensitivity and specificity (31). Indeed autoantibodies are considered ideal biomarkers for early detection of many diseases since their presence may signal a pre-clinical phase of the disease (32).
In conclusion, the APS-90 detected 29 autoantibodies in the human plasma samples we analyzed, all of which are relevant in autoimmune disorders. Among them, 4 autoantibodies were present at significantly different levels between the test (ovarian cancer) and reference (no cancer) groups. Although intriguing, no definitive conclusions can be drawn regarding the potential use of these autoantibodies as ovarian cancer biomarkers because of the small sample size. The present study however demonstrates that it is possible to screen a plasma sample with a low-density antigen array for the purpose of determining the presence/absence of autoantibodies. If validated, this relatively fast, simple and inexpensive method could be a first-level screening paradigm to test for multiple autoantibodies as an aid to diagnosis and treatment planning.
Acknowledgements
This study was supported in part with grants from the National Institutes of Health (NIH R01-CA-106414), American Cancer Society (CRTG-00-196-01-CCE) and the Department of Defense Advanced Cancer Detection Center Grant (DAMD-17-98-1-8659) received by Dr Rebecca Sutphen for the Tampa Bay Ovarian Cancer Study.
- Received July 27, 2015.
- Revision received October 6, 2015.
- Accepted October 15, 2015.
- Copyright© 2016, International Institute of Anticancer Research (Dr. John G. Delinasios), All rights reserved