

Abstract
Background: Colorectal cancer (CRC) is the third most common type of cancer and the fourth most frequent cause of cancer death. Literature indicates that vascular endothelial growth factor is a predominant angiogenic factor and that angiogenesis plays an important role in the progression of CRC. Patients and Methods: The present series consisted of tissue samples obtained from 672 patients who had undergone large bowel resection between 2005 and 2010 at the Braga Hospital, Portugal. Archival paraffin-embedded CRC tissue and normal adjacent samples were used to build up tissue microarray blocks and VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expression was immunohistochemically assessed. Results: We observed an overexpression of VEGF-C in CRC when tumour cells and normal-adjacent tissue were compared (p=0.004). In tumour samples, VEGF-C-positive cases were associated with VEGFR-3 expression (p=0.047). When assessing the correlation between VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expressions and the clinicopathological data, it was revealed that VEGF-A positive cases were associated with male gender (p=0.016) and well-differentiated tumours (p=0.001); VEGF-C with colon cancers (p=0.037), exophytic (p=0.048), moderately-differentiated (p=0.007) and T3/T4 (p=0.010) tumours; VEGFR-2 with invasive adenocarcinoma (p=0.007) and VEGFR-3 with the presence of hepatic metastasis (p=0.032). Overall survival curves for CRC were statistically significant for rectal cancer, VEGF-C expression and stage III (p=0.019) and VEGFR-3 expression and stage IV (p=0.047). Conclusion: Quantification of VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expression seems to provide valuable prognostic information in CRC and the correlation with clinicopathological data revealed an association with characteristics that contribute to progression, invasion and metastasis leading to poorer survival rates and prognosis.
- Colorectal cancer
- vascular endothelial growth factor
- clinical and pathological data
CRC: Colorectal cancer; VEGF: vascular endothelial growth factor; TMA: tissue microarray; NAE: normal adjacent epithelium.
Colorectal cancer (CRC) is the third most common type of cancer (1-4) and the fourth most frequent cause of cancer death (1-5). Globally, CRC incidence varies widely, with higher rates in North America, Australia and western Europe, and the lowest rates in developing countries (4, 6), although in recent years, increasing CRC rates have been reported in these countries (4, 7). According to the World Health Organization (WHO), CRC is one of the most prevalent diseases of the occident world (4, 8) and the second most common cause of death from malignant diseases in Western countries (4, 9, 10). Despite improvements in treatment, mortality remains high, with metastatic spread to the liver occurring in approximately 50% of patients (10). In Portugal, data from Statistics Portugal revealed that CRC is the second most common type of cancer, after gastric cancer, with an incidence of 5,000 individuals year and one of the main causes of death from neoplastic disease (11).
Detailed aspects of the immunohistochemical procedure used to visualize the different proteins.
Angiogenesis plays a key role in tumorigenesis and metastatic processes (1, 12, 13). It consists of the formation of new blood vessels from the endothelium of pre-existing vasculature (2, 13). Tumour angiogenesis is essential for neoplastic mass development, favouring access to the blood components and also strengthening the vascular routes in the metastatic process (14-16). Neovascularisation as a whole, promotes tumour growth by supplying nutrients, oxygen and releasing growth factors that promote tumour cell proliferation (13, 14, 17-19).
Numerous studies have demonstrated that tumour overexpression of vascular endothelial growth factor (VEGF) is associated with advanced tumour stage or tumour invasiveness in various types of common human cancer (13, 20-22), and its overexpression in colonic cancer tissue indicates poor prognosis (22); although paradoxically, some data showed that VEGF has no significant prognostic value in colon cancer tissue (23). VEGF-A is the most widely studied angiogenic factor; it increases vascular permeability and is the main angiogenic protein known (4, 12, 19-20, 23-25).
In this study, we evaluated the expression of VEGF-A, VEGF-C, and their receptors VEGFR-2 and VEGFR-3 in a series of 672 cases and determined their correlation with clinicopathological parameters.
Materials and Methods
Data from 672 patients treated in the Braga Hospital, North of Portugal, between January 1st 2005 and January 1st 2010 with CRC diagnosis and submitted to surgical treatment was collected prospectively. The data collected from clinical and preoperative diagnostic examinations included: age, gender, clinical presentation, oncologic history, tumour localization, histological type, macroscopic appearance and preoperative staging. The tumour localization was recorded and classified as colon and rectum (between anal verge and 15 cm at rigid rectoscopy). Operative reports made by surgeons included data such as the presence of perforation; information about tumour mobility and type of surgery was also collected. Histopathological reports included: tumour extent (T), extent of spread to the lymph nodes (N), presence of distant metastasis (M), tumour differentiation, resection margins involvement and lymphatic and blood vessel invasion. The level of positive lymph nodes was not described in all specimens. The histological type of CRC was determined by two experienced pathologists and tumour staging was graded according to the TNM Classification of Malignant Tumours (TNM), sixth edition (25).
Pattern of protein staining in tumour versus normal adjacent epithelium (NAE). *Examined for statistical significance using the Fisher’s exact test (when n<5).
A series of formalin-fixed, paraffin-embedded tissues from these patients was analyzed by immunohistochemistry for VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expression. Slides from all 672 specimens were reviewed and mapped and tissue microarrays were built using a manual tissue arrayer (MTA-1 Beecher Instrument, Silver Spring, MD, USA). Representative areas of the CRC lesions were selected and cores of 1.0 mm in diameter were twice-sampled and arranged at 0.3 mm from each other in the recipient paraffin block. A database was built for every block produced, including the coordinates of each core and case of origin. Comparison of expression in tumour versus normal cells was also possible since, in most cases, the same paraffin section contained both neplastic and normal colonic epithelium. VEGF immunohistochemical expression was correlated with the available clinicopathological data. All cases in this study were identified using a series of unified codes, for the following review. The study protocol was approved by the Ethics Committee of the Braga Hospital.
Assessment of associations between expression of VEGF-A and VEGF-C and the receptors VEGFR-2 and VEGFR-3 in tumour cases.
Assessment of correlation between VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expression and clinical data. *Examined for statistical significance using Fisher’s exact test (when n<5).
Immunohistochemistry. Tissue microarray (TMA) protein expression was evaluated by immunohistochemistry. Briefly, after deparaffinization and rehydration, 3 μm sections were immersed in 0.01 M citrate buffer (pH 6.0) and heated at 98°C for 20 min for epitope antigen retrieval. Subsequently, endogenous peroxidase was blocked with 0.3% hydrogen peroxide in methanol. The primary antibody incubation step take place overnight at 4°C. Visualization was developed with 3,3’-diaminobenzidine (DAKO Corporation, Carpinteria, CA, USA) and counterstaining with Harris’s haematoxylin (Merck, Dermstadt, Germany). Negative controls were obtained by omitting the primary antibody incubation step and tonsils were used as positive control.
Details of the procedure used for each antibody are found in Table I. After the immunohistochemical procedure, the slides were evaluated and then photographed under a microscope.
Immunohistochemical evaluation. Sections were scored semiquantitatively for the extent of immunoreaction as follows: 0: 0% of immunoreactive cells; 1: <5% of immunoreactive cells; 2: 5; 50% of immunoreactive cells; and 3: >50% of immunoreactive cells. The intensity of staining was scored semi-qualitatively as 0: negative; 1: weak; 2: intermediate; and 3: strong. The final score for the immunoreaction was defined as the sum of both parameters (extent and intensity), and grouped as negative, 0, weak, 2, moderate, 3, and strong, 4;6. For statistical purposes, only the moderate and strong immunoreaction final scores were considered as positive. Evaluation of VEGF immunohistochemical expression was performed blindly by two independent observers and discordant cases were discussed under a double-head microscope in order to determine a final score.
Statistical analysis. All data were collected and stored in an Excel PC database and statistically analyzed using the Statistical Package for the Social Sciences, version 19.0 (SPSS Inc., Chicago, IL, USA). All comparisons were examined for statistical significance using Pearson’s chi-square (χ2) test and the Fisher’s exact test (when n<5), with the threshold for significant p-values of less than 0.05. Survival curves were determined for overall survival by the Kaplan-Meier method.

Immunohistochemical expression of VEGF-A, VEGF-C, VEGF-R2 and VEGF-R3 in colorectal cancer samples (original magnification ×40).
Assessment of correlation between VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expression and diagnostic/surgical data. *Examined for statistical significance using Fisher’s exact test (when n<5).
Results
VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expressions in CRC samples. A total of 672 samples were organized into TMAs, including tumour and normal adjacent epithelium (NAE). Sections were evaluated for immunoexpression and the obtained results are given in Table II, which summarizes the frequency of VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expression in tumour cells and NAE.
When analyzing the results of Table II, it can be seen that only VEGF-C is overexpressed in tumours when tumour cells and NAE are compared (p=0.004), and VEGFR-2 shows a tendency to be differently expressed (p=0.064).
Figure 1 shows representative cases of positive staining for VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 in tumour cells and in NAE.
Associations between VEGF-A, VEGF-C and VEGFR-2, VEGFR-3 expression in CRC tissues. We analyzed the associations between the expression of VEGF-A, VEGF-C and the receptors VEGFR-2 and VEGFR-3 in CRC tissues and observed that in the tumour samples, VEGF-C positivity was associated with VEGFR-3 positivity (p=0.047) (Table III).
Associations between VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expressions in CRC tissues and clinical data. An assessment of the correlation between the expression of VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 and the clinical data revealed that VEGF-A-positive cases were less frequently associated with female gender (p=0.016) and VEGF-C had a tendency to be associated with a personal history of CRC (p=0.060) Table IV.
When analyzing the correlation with data from diagnosis/surgery, we found an association between VEGF-C expression and tumour localized in colon (p=0.037) and a exophytic macroscopic cancer appearance (p=0.048). VEGFR-3 shows an association with the presence of hepatic metastasis’ (p=0.032) Table V.
Assessment of correlation between expression of VEGF-A, VEGF-C, VEGF-R2 and VEGF-R3 pathological data. *Examined for statistical significance using Fisher’s exact test (when n<5).
When analysing the correlation with pathological data, we found an association between the expression of VEGF-A and well-differentiated tumours (p=0.001); VEGF-C and moderately-differentiated (p=0.007) and T3/T4 penetration tumours (p=0.010); VEGFR-2 expression and invasive adenocarcinoma (p=0.007) Table VI.
Overall survival curves according to expression of VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3. A statistically significant association between VEGF-C expression and stage III rectal cancer (p=0.019) and VEGFR-3 expression and stage IV rectal cancer (p=0.047) was found Figures 2, 3, 4, 5, 6, 7.
Discussion
Our results corroborate the premise that angiogenesis plays a key role in tumourigenesis and metastatic processes (1, 12, 13), because all the markers involved in neovascularization were consistently expressed in tumour cells. Additionally, VEGF-C, a lymphangiogenic marker was significantly overexpressed in cancer cells rather than in normal counterparts. This general view of our results clearly indicates that CRCs are predominantly composed of cancer cells that are directly or indirectly associated with the high expression of molecules related to blood neovascularization (angiogenesis) and that the major lymphangiogenic molecules are also importantly expressed in cancer cells.
Normally, the VEGF family is weakly-expressed in a wide variety of human and animal tissues; however, high levels of VEGF expression can be detected at sites where physiological angiogenesis is required, such as foetal tissue or placenta and in a vast majority of human tumours and some other diseases e.g. chronic inflammatory disorders, diabetes mellitus, and ischemic heart disease (4). Furthermore, both the VEGF family and its receptors are expressed at high levels in metastatic human colon carcinomas and in tumour-associated endothelial cells, respectively (4, 20). Consequently, VEGF is recognized as a prominent angiogenic factor in colon carcinoma and the assessment of VEGF expression may be useful in predicting metastasis from CRC (4, 20). In fact, VEGF-A expression was found to be higher in patients with metastatic tumours than in those with non-metastatic tumours (4, 20, 26), and high levels of VEGF-A expression were associated with advanced cancer stage and related to an unfavourable prognosis (4, 22, 23, 27). Other studies have shown that VEGF-A is also a useful marker for prognosis by significantly correlating with angio-lymphatic invasion, lymph node status and depth of invasion, although it was not an independent prognostic factor (4, 14, 24).

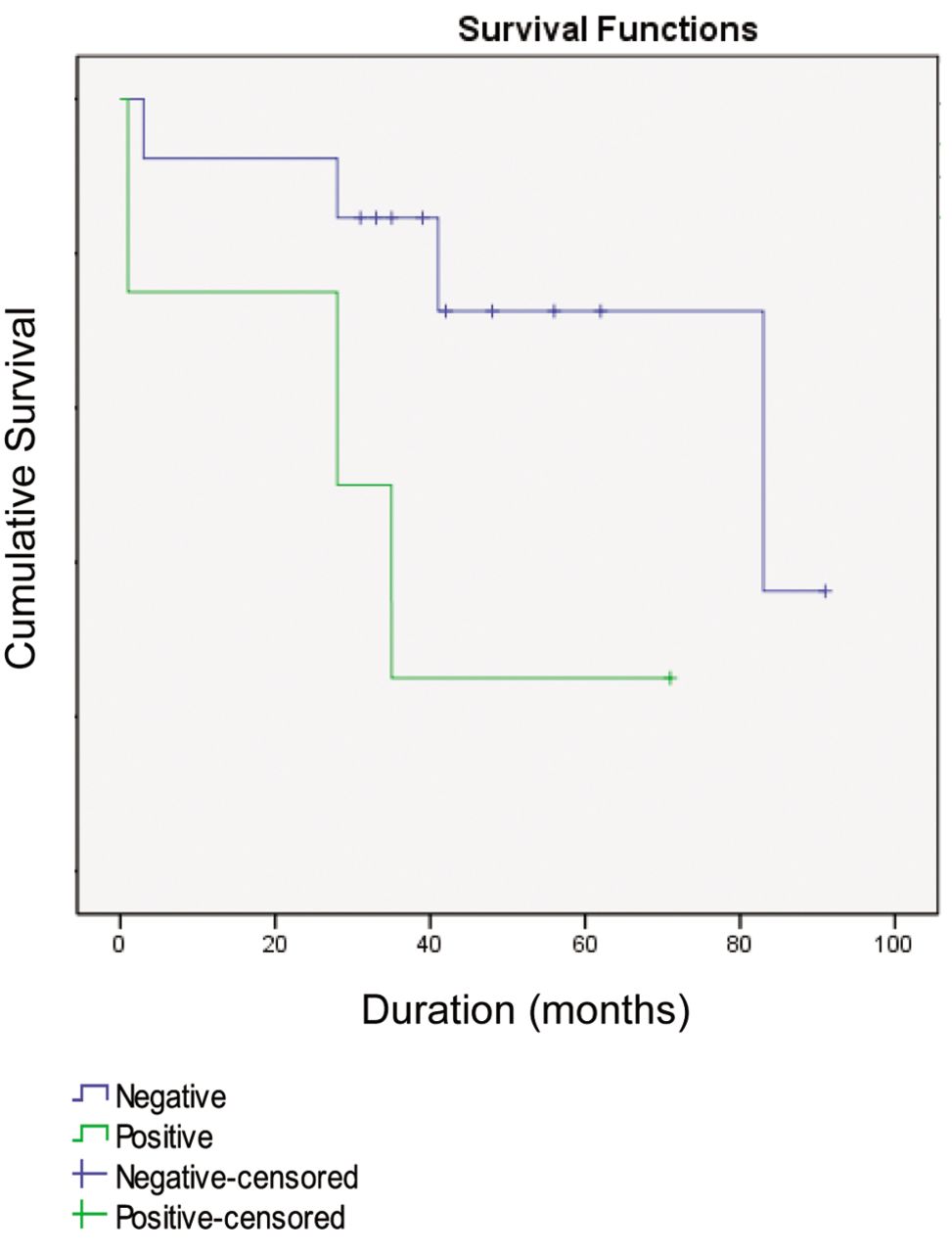
Survival curve of patients with stage III rectal cancer according to VEGF-C expression, assessed by the log-rank test (p=0.019).
The effect of VEGF depends not only on tumour cell expression of VEGF, but also on that of VEGF-R in the endothelial cells (4, 13). The ligands of the VEGF family include VEGF-A, VEGF-B, VEGF-C, VEGF-D and VEGF-E; and the receptors are VEGFR-1, -2 and -3 (4, 28).
In literature, the role of the VEGF family members in CRC has, to date, mainly concentrated on VEGF-A, but the newer members of the family, VEGF-C and VEGF-D, may have important roles to play in both angiogenesis and lymphangiogenesis (29).
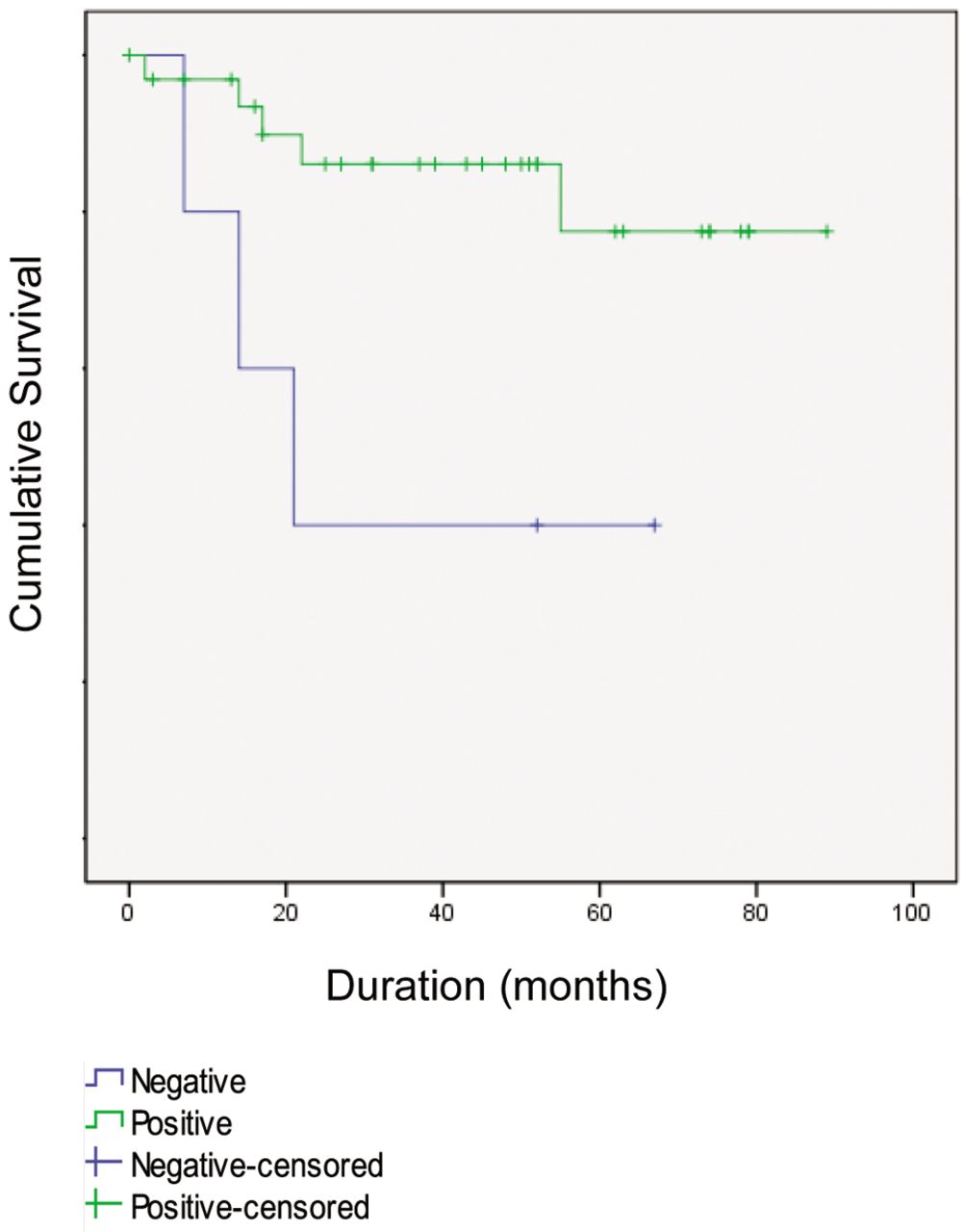
Survival curve of patients with stage IV rectal cancer according to VEGFR-3 expression, assessed by the log-rank test (p=0.047).
VEGF-A promotes angiogenesis through enhancement of permeability, activation, survival, migration, invasion, and proliferation of endothelial cells (4, 30). VEGF-A plays a role in early tumour development at the stage of adenoma formation (4, 10, 31) and some studies documented an overexpression of VEGF-A in CRC (4, 24).
The VEGF-C gene was also found to be poorly expressed, with only moderate overexpression in CRCs compared to control tissues (29, 32); however, the number of samples studied was very small (n=12). In a larger series of patients, the immunohistochemical expression of VEGF-C was correlated with lymph node spread (29, 33). In our study, contrary to what is found in literature, we did not observe a statistically positive relation between VEGF-A expression in tumours and NAE. We observed that VEGF-C is overexpressed in tumours when comparing tumour cells with NAE (p=0.004), and VEGFR-2 shows a tendency for a similar association (p=0.064).
We also analyzed the associations between expression of VEGF-A, VEGF-C and the receptors VEGFR-2 and VEGFR-3 in CRC tissues and observed that in tumour samples, VEGF-C positivity was associated with VEGFR-3 expression (p=0.047); this is consistent with the results mentioned above, where lymphangiogenesis induced by VEGF-C is driven mainly by the activation of the tyrosine kinase-linked receptor VEGFR-3 (34). This receptor occurs in embryonic vascular endothelial cells, where its production decreases during development and is subsequently restricted to lymphatic vessels after vascular net formation (35). Many experimental studies have indicated that VEGFR-3 and its ligands (VEGF-C and -D) stimulate lymphangiogenesis in tumours and induce proliferation and growth of new lymphatic capillaries, enhancing the incidence of lymph node metastasis (36-40).

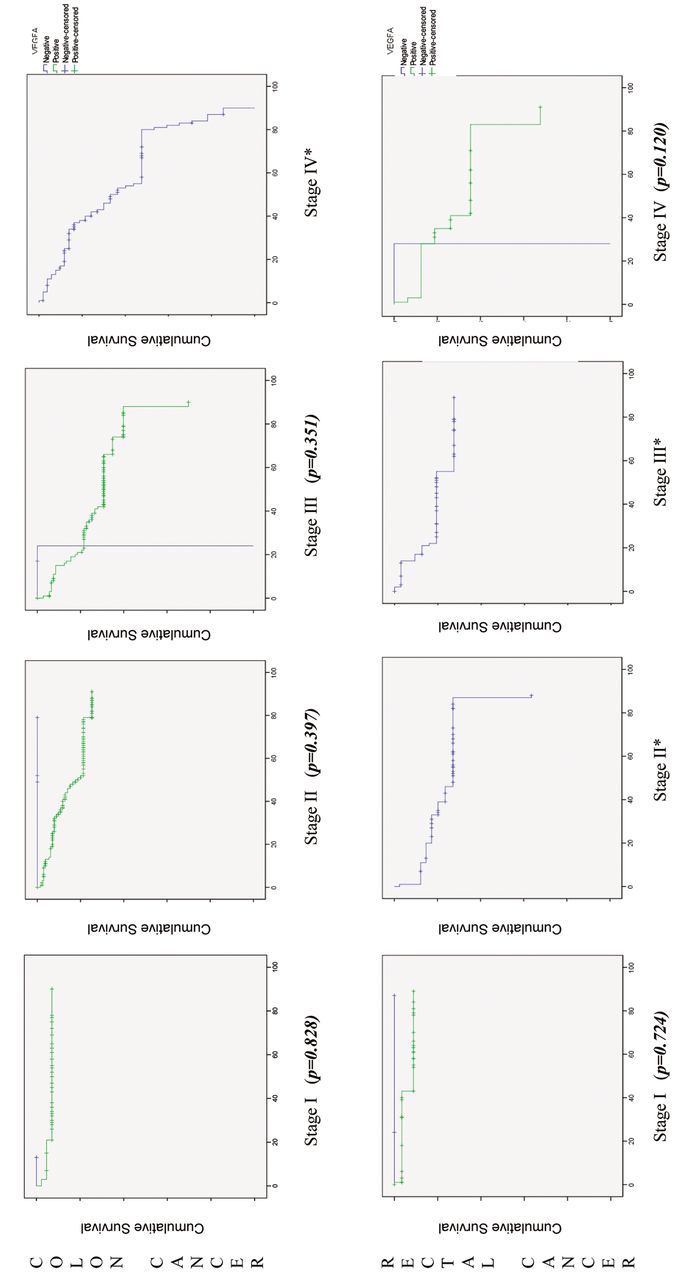
Survival curve of patients with different stages of colorectal cancer according to VEGF-A expression, assessed by log-rank test. *No comparison was possible, because all cases were VEGF-A-positive.

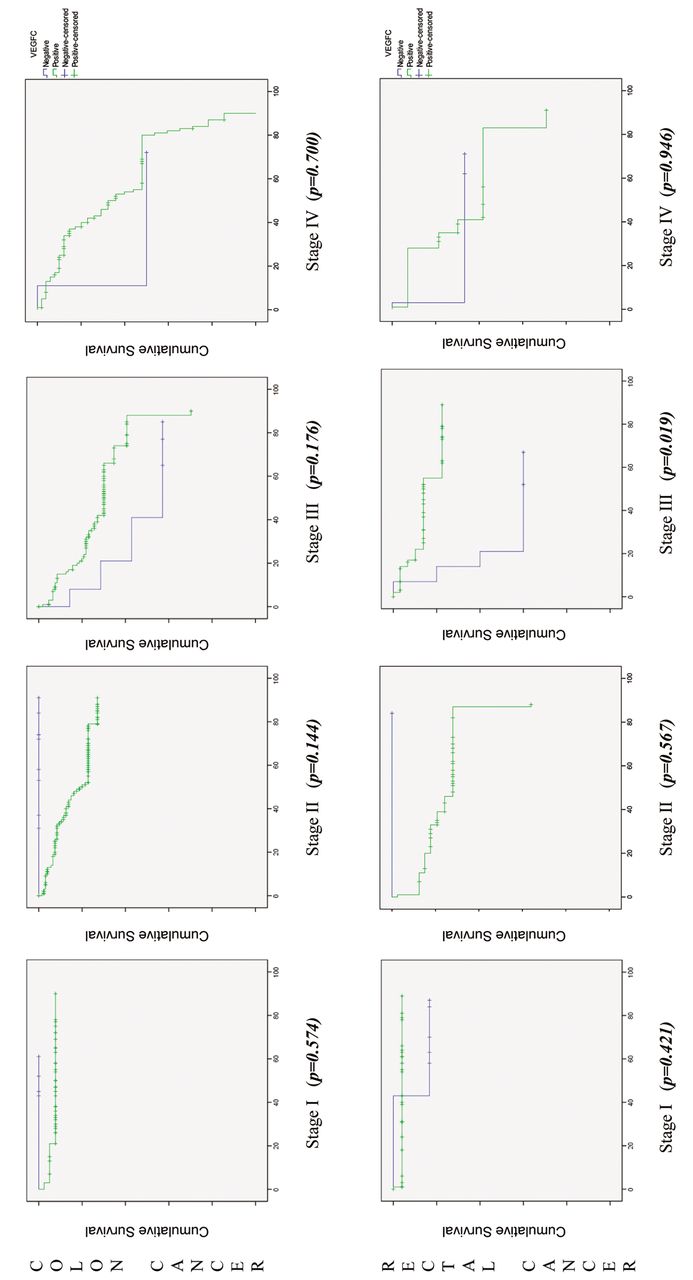
Survival curve of patients with different stages of colorectal cancer according to VEGF-C expression, assessed by the log-rank test.

Survival curve of patients with different stages of colorectal cancer according to VEGFR-2 expression, assessed by log-rank test. *No comparison was possible, because all cases were VEGFR-2-positive.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival curve of patients with different stages of colorectal cancer according to VEGFR-3 expression, assessed by the log-rank test.
The comparison of VEGF-A, VEGF-C, VEGFR-2 and VEGFR-3 expressions and the clinicopathological data, data from diagnosis/surgery and pathological data revealed that VEGF-A-positive cases were associated with male gender (p=0.016) and well-differentiated tumours (p=0.001); VEGF-C expression with cancers localized in colon (p=0.037), exophytic (p=0.048), moderately-differentiated (p=0.007) and T3/T4 penetrating tumours (p=0.010); VEGFR-2 shows an association with invasive adenocarcinoma (p=0.007) and VEGFR-3 with the presence of hepatic metastasis (p=0.032). All of these characteristics contribute to progression, invasion and metastasis, and poorer survival and prognosis, as stated in literature to be associated with VEGF-A overexpression in CRC (4, 30). Moreover VEGF-C overexpression in CRC has been found to correlate with lymphatic invasion and lymph node metastasis (41). Increased VEGF-C mRNA expression in tumour tissues was also documented to be positively correlated with lymphatic metastasis and poor prognosis (42). In our series, we reported significantly poor survival when we correlated overall survival with VEGF-C in stage III rectal cancer (p=0.019) and VEGFR-3 expression in stage IV (p=0.047).
Footnotes
-
Competing Interests
We declare no financial or non-financial competing interests.
- Received February 11, 2013.
- Revision received March 6, 2013.
- Accepted March 6, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinasios), All rights reserved