


Abstract
Background: When a protein has a useful and unique function, the selective pressures of evolution conserve the DNA sequences encoding such proteins; the conservation of these domains may have pragmatic use in better understanding viral and spontaneous carcinogenesis in eukaryotic cells. The unique functions of ribosomal protein (RP) Metallopanstimulin-1 (MPS-1/RPS27), and a few other RPs, in growth regulation and carcinogenesis (chemical, viral, radiation and chemotherapy-induced) could be used for the early detection of cancer using serum, or in follow-up therapy. Materials and Methods: The MPS-1 serum test was performed in the serum of patients by radioimmunoassay using specific antibodies directed against the N-terminus (amino acids 2 to 17; synthetic peptide) of MPS-1 according to previously described procedures (Fernandez-Pol, JA, 1994). Results: The data presented here indicate that antibodies to MPS-1 detect a zinc finger protein of Mr 9.8 kDa identified by MS and sequencing as MPS-1 in patients having various types of cancer. MPS-1 increases with aggressivity of cancer, irrespective of the cancer types studied in this work. In healthy individuals of the same age range, the levels of MPS-1 increase slowly and progressively at less than 1% per year as the patients age. Conclusion: The MPS-1 test may be useful as an aid in: i) early detection of a wide variety of cancer types; and ii) the prognosis and management of cancer patients by following the changes in the concentrations of MPS-1 in serum. Moreover, the results suggest that the combined use of MPS-1 with physical methods of cancer detection such as positron emission tomography, computer assisted tomography, or magnetic resonance imaging techniques may significantly improve the chances of identifying an active tumor in early stages by serodiagnosis of MPS-1. In patients having other diseases (such as rheumatoid arthritis, which manifests as a proliferative disease) or in healthy individuals having no evidence of disease, the identification of as yet unrecognized active oncogenesis, may be significantly improved by using MPS-1. The data on genome context analysis indicates that the presence of MPS-1 in the blood is an indicator of oncogenesis. Thus, the test may be used to help prolong the life of the patients, if the cancer is detected early.
- Metallopanstimulin-1
- RPMPS-1/RPS27
- p53
- DNA repair protein
- RP
- ribosomal protein
- breast cancer detection
- zinc finger proteins
- oncogenesis
- tumor marker
- growth factors
Metallopanstimulin-1 (MPS-1) is a ribosomal protein (RP) S27, and thus also denoted in gene banks as RPMPS-1/S27 (which is the intracellular form). MPS-1, (which is the extracellular form present in the serum), is a 9.8-kDa subunit zinc finger protein which is expressed in a wide variety of actively proliferating normal cells and in aggressive malignant neoplastic tissues (1-9). Experimental translation from basic science research to clinical science and important milestones in the characterization of this multifunctional protein are briefly described in Table I, which refers to experiments performed in the laboratories of Fernandez-Pol, from 1989 until 1999. An important finding of MPS-1 in gastric cancer progression and carcinogenicity is that of Yun-wei et al. (10). A remarkable recent finding is that of Xiong et al. indicating that ribosomal protein RPMPS-1/S27 and S27-like interplay with the p53-MDM2-axis as a target and regulator of oncogene expression (11). The authors believe that the data indicates that the chances of eradicating cancer in general are significantly higher than previously thought, as new targets that regulate DNA repair have been recently identified (6, 8, 11, 12).
RPMPS-1/S27 is a ribosomal protein that is over-expressed in many cancer cell lines, in most cancer tissue biopsies, and is increased in the serum of patients with early stage cancer (8). Previous work by Fernandez-Pol with cancer cells utilizing gene cloning (1, 2, 8) and Berthon et al. (12) with Archaea utilizing genome context analysis, showed that RPMS-1/S27 is involved in translation, transcription, DNA repair, and ribosomal biogenesis. In normal aging cells, the level of RPMPS-1/S27 decreases when the cells age and reach the senescent stage (13). Initially, its expression was found to be increased in transformed cells in tissue culture (8).
Translating basic research in the clinic: important milestone that lead to the development of the RPMPS-1/S27 test for the early detection of cancer in the human sera.
As a result of the over-expression of RPMPS-1/S27 (8), a derivative of this protein, denoted MPS-1, is released from the tissues into the blood stream where it can be detected in the sera by sensitive techniques (6, 8). Furthermore, Fernandez-Pol et al. (5) demonstrated the potential of MPS-1 as a tumor marker in the serum for numerous different types of cancer (5, 8). Elevated MPS-1 levels and derivatives thereof were identified in cancer patients with greater than 90% confidence limits (8). In healthy individuals, not having malignant neoplastic disease previously, the MPS-1 levels were <10 ng/mL (>99% of a random population from 20 to 70 years of age). In untreated cancer patients, the MPS-1 level ranged from 15 to 50 ng/mL and in stage M1b (metastasis to the bones) the MPS-1 levels were extremely high (>100 to 1000 ng/mL). In M1b patients that did not respond to therapy, the MPS-1 levels remained very high (>100 ng/mL). In those patients that went into remission after treatment, the MPS-1 levels were reduced by >50-70% at 2 months post-treatment. The converse is also true: when the level of MPS-1 increases it can be predicted with >95% accuracy that the tumor relapse, allowing the oncologist to treat the tumor earlier (9).
This suggests that the MPS-1 test may be useful as an aid in: i) the early detection of a wide variety of neoplastic conditions; and ii) for the prognosis and management of cancer patients by following the changes in the concentrations of MPS-1 in serum. It is germane to point out here that the results indicate that both the combined use of MPS-1 in serum with physical methods of cancer detection such as computer assisted tomography (CAT), positron emission tomography (PET), or magnetic resonance imaging (MRI), can significantly improve the chances of detecting active oncogenic processes in their earlier stages. Furthermore, in patients having other diseases (such as rheumatoid arthritis which manifests as a proliferative disease of abnormal synovial cells) or in healthy individuals having no evidence of cancer or other diseases, the use of MPS-1 measurement may significantly improve the probability of early detection of active carcinogenesis not previously recognized by other diagnostic techniques. Finally, early diagnosis of cancer using the MPS-1 test may be economically beneficial especially if the test is combined with physical techniques (CAT, PET, MRI).
Intracellular RPMPS-1/S27 participates in critical homeostatic mechanisms and, when altered by the carcinogenic process, is released into the extracellular space and from there into the serum as MPS-1 (5-9).
This paper presents a large number of measurements in more than 2500 individual patients with many types of common cancers. It was decided to present individual patients in a summarized form obtained from complete computerized clinical charts, so if the reader wishes he or she can carry out from simple to more complex statistics, to evaluate the consistency of the data. This can be easily done as the values correspond to individual measurements of samples. It is believed that MPS-1 serum protein is a sensitive and reliable marker of detecting proliferative diseases, including benign, and malignant tumors, and non-malignant proliferative diseases.
Materials and Methods
Patients. This retrospective study (Tables II, III, IV, V, VI, VII, VIII, IX, X, XI, XII, XIII and XIV) was carried out on different types of patient samples measured in duplicate. Diagnosis was based on detailed computerized clinical history, including laboratory information, pathological diagnosis with various staining procedures for oncogenes, radiological information (CAT, PET, MRI, and Ultrasound), staging of cancer, treatment plan, results, chemotherapy protocols, radiation therapy and surgical procedures. Tumor registry information was also available. This research adheres to the principles of the Declaration of Helsinki.
As shown in Tables II, III, IV, V, VI, VII, VIII, IX, X, XI, XII, XIII and XIV, the clinical study consisted of individuals separated into healthy individuals, and individuals with active cancer of different types. Other malignancies category reflects individuals, who had cancer with unknown origin. The mean age of the group was 70±10 years, with a range of 19 to 100 years.
Analysis of human blood samples. The majority of the specimens consisted of discarded samples obtained from the Laboratory of Virology and Immunology, DVA Medical Center JC, St Louis, MO, USA (DVA Med. Ctr.). The use of residual blood samples was approved by the Human Research Studies Subcommittee, DVA Medical Center, as “Research Exempt from IRB (Internal Review Board) Review”, in accordance with the USA FDA regulations CFR-21. Other samples were controls purchased from various commercial reference laboratories such as Nichols, CA, USA, Sigma-Aldrich, (St, Louis, MO USA, or Bioclinical Partners, Boston, MA, USA, and also from healthy individual volunteers who signed the proper written consents as required by the IRB of the DVA Med. Ctr., St Louis, MO, USA.
The serum samples corresponding to both healthy females and females with breast cancer in different stages of progression (0 to IV) were purchased from reference laboratories (Bioclinical Partners, Boston, MA, USA, and Nichols Laboratories, San Juan Capistrano, CA, USA).
Preparation of reagents. The critical reagents used for the MPS-1 Radioimmunoassay (RIA) serum test, were all made in the Laboratory of Molecular Oncology (DVA Med. Ctr., St. Louis MO, USA) and consisted of human recombinant MPS-1 protein (as an MPS-1 RIA control), synthesized in our laboratory from plasmid STIH2 in a Baculovirus insect system (2). The polyclonal antibodies to recombinant MPS-1 were created in this laboratory in rabbits. The use of rabbits was approved by the R & D Committee and the animals were supervised by the Board Certified Veterinarians of the Animal Research facility. Affinity chromatography purified polyclonal antibodies were prepared, characterized and, verified for quality control according to methods described elsewhere (2). The standard of reference for the MPS-1 RIA test was the Baculovirus-produced human MPS-1 recombinant protein (2). The RIA MPS-1 test used the MPS-1 Peptide-N-terminus (AA 2-17) of MPS-1. The Peptide (AA-2-17) was synthesized by Fmoc chemistry and was used to generate antibodies to Peptide (AA-2-17) in rabbits. The synthesis was verified by electrospray Mass Spectrometry (Protein and Nucleic Acid Chemistry Laboratory, Washington University, St. Louis, MO USA). The antibody is directed towards a unique site on the MPS-1 molecule (AA 2-17). The polyclonal antibodies were purified by affinity chromatography.
Radioimmunoassay procedure. The RIA used in the present research is based on the following US patents by Fernandez-Pol: (i) DNA vector with isolated cDNA gene encoding Metallopanstimulin (MPS-1), US. Pat. No. 5,243,041; (ii) Method of preparing and activating samples for RIA and other test, US Pat. No. 5,668,016; and Method of determining biological substances elevated in the presence of cancer and other neoplasms, US Pat. 5,955,387. These patents are hereby incorporated by reference. These patents contain in full detail the following numerical data and analysis: Distribution of MPS-1 values in human serum, the essential materials and sources, the stability, controls, preparation of reagents and sources, specimen collection and preparation, and preparation of samples for RIA. The RIA procedure in full numerical detail is presented in US Pat. 5,668,016, including: special considerations, data, calculations and RIA standard curve, quality control, drift values, parallelism and immunological identity, recovery, expected values, false positive and false negative results in various biological conditions, serum protein/MPS-1 relationship, and false positives.
The effect of boiling time on the measurement of MPS-1 in healthy individual's serum and cancer patient's serum is shown in Figure 1. In healthy individuals the serum MPS-1 barely increases after boiling while the MPS-1 molecule in metastatic cancer patients show a peak at 3 minutes at 100°C of about 1000 ng/mL of MPS-1, indicating the release of MPS-1 from a serum carrier protein of Mr 90 kDa.
Methods to evaluate apoptosis and MPS-1 indices in malignant cells of the skin to estimate the release of MPS-1 in adjacent tissues and into serum. To assess the relative frequency of MPS-1 expression in individual cells and apoptosis in cells, malignant melanoma of the skin was used due to its high production of MPS-1 protein. Immunohistochemistry of MPS-1 and tunnel methodology for estimation of apoptosis was carried out in x, y and z Cartesian coordinates using specific software to analyze the slides to enable the generation of 3D images utilizing the Jurassic Park, Silicon Valley Computer and the corresponding 3D programs.
Protocols for detecting MPS-1 staining and apoptosis in formalin fixed sections were previously described (14, 15). For apoptosis, slides were stained using a commercially available kit denoted Frag El-Klenow DNA Fragmentation Detection Kit from Oncogene Research Products, Cambridge, MA, USA. One of the characteristics of apoptotic cell death is specific fragmentation of DNA. The details of the method are described elsewhere (8).
Statistical analysis. The RIA MPS-1 assay was evaluated for sensitivity, specificity, positive predictive value, negative predicted value, diagnostic accuracy, and the cutoff index to identify the optimum threshold level and assess its efficacy in the diagnosis of neoplasia. Differences between groups were identified with the Chi-square test for contingency tables and for standard deviation (14, 15). P<0.05 was defined as being statistically significant. Processing was carried out using the statistical functions provided by Excel (Microsoft Corp.). Correlation between MPS-1 levels versus the presence or absence of proliferative conditions was done using scatter plots for different values of the sample (15), the USA FDA approved guidelines for RIA (14), evaluation of diagnostic tests (16), and the method of Sackett et al. (16, 17). Quality control for RIA standard curves was carried out by the classical RIA Levy-Jennis plots to verify ±SD and ±SE, to determined compliance of the measurements (5,14). Full numerical details of all the procedures denoted above are presented in US. Pat. No. 5,668,016 and US. Pat. No. 5,955,387, containing also in detail the sources of the materials used in RIA and of the instruments used.
Results
Performance characteristics of the RIA MPS-1 assay. The reliability of the MPS-1 RIA procedure was evaluated by examining the reproducibility of measurements on selected reference samples that represent the range of values most frequently found in human sera (2-500 ng/mL). The results showed that: (i) the intra-assay precision was <12%; (i) the inter-assay precision was <13%; and (iii) the sensitivity, or minimal detectable dose, was approximately 2 ng/mL.
Measurement of circulating MPS in sera of patients evaluated for cancer.
Expected values. The relative distribution of MPS-1 concentrations in healthy individuals, patients with various types of active cancer, and patients with non-malignant diseases is presented in Tables II, III, IV, V, VI, VII, VIII, IX, X, XI, XII, XIII and XIV, and also illustrated graphically from data extracted from each Table (II, III, IV, V, VI, VII, VIII, IX, X, XI, XII, XIII and XIV), to facilitate interpretation of the results for cancer patients in stable conditions, in progression, or remission, which is not possible to easily deduce from simply examining the numerical tables with fully processed data alone.
Healthy individuals: The results of studies with healthy individuals indicate an MPS-1 reference range for adults (<70 years) of non-detectable to 10 ng/mL (98%) of the healthy population). A total of 2% of this group had MPS-1 levels in the range of 10.01-20.0 ng/mL (designated as the intermediate grey area because of significant overlapping with both active cancerous disease and non-malignant conditions at this range. Tables II, III, IV, V, VI, VII, VIII, IX, X, XI, XII, XIII and XIV show the plots and the range levels corresponding to various types of cancer. There was no significant difference in MPS-1 levels between female (19-70 years) and male (21-88 years) healthy individuals.
Biological and physiological characteristics of MPS-1 in human normal and malignant tissues and serum as detected with polyclonal antibodies against MPS-1 (AA 2-17 peptide) and methods to detect apoptosis. To initially illustrate the characteristics of MPS-1 as a tumor marker, a few examples are presented in the following section before the extensive analysis of the serum samples of individual patients are presented in Tables II, III, IV, V, VI, VII, VIII, IX, X, XI, XII, XIII and XIV.
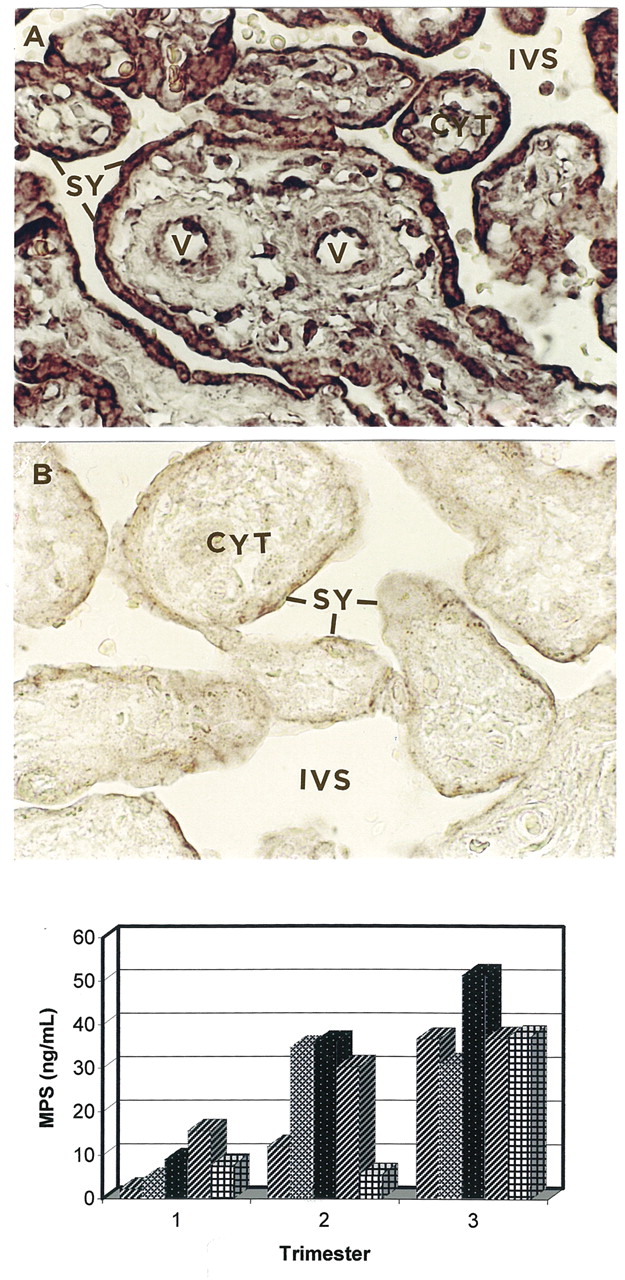
Presence of MPS-1 in syncytiotrophoblasts (SY) and its release into the blood of pregnant women (Figure 2). Syncytiotrophoblasts are multinucleated cells found in the placenta of embryos. They are the outer syncytial layers of the trophoblasts and actively invade the uterine wall and blood vessels. In this sense they behave as invasive cancer cells. Cells from the syncytiotrophoblasts secrete MPS-1 in the blood vessels of pregnant women and thus, MPS-1 can be detected in the circulation. Figure 2A shows SY stained with anti-MPS-1 antibodies, while Figure 2B shows anti-MPS-1 antibody neutralized by 100-fold peptide A (2-17 domain of MPS-1), showing neutralization of the antibody staining, indicating specificity. Figure 2C, bottom chart, shows that the MPS-1 level in the serum measured by RIA, of five separate healthy pregnant women increases in a time-dependent fashion with the 1st, 2nd and 3rd trimester, of pregnancy as the syncytiotrophoblast progressively invades the uterus.

The effect of boiling time on the measurement of MPS-1 in patient's serum. MPS-H, heat-activated MPS-1 protein in the serum. The serum samples were boiled to 100°C for the times indicated in the abscissa. Ordinate, ng/mL of released MPS-1 protein from the serum after heat treatment.
MPS-1 identified by immunoblot studies in serum of a cancer patient, and in serum of a healthy individual with no evidence of cancer (Figure 3A). The serum was obtained from a patient with metastatic cancer. Peaks 4 and 5 correspond to MPS-1 [4], and peak [5] to a degradation product of MPS-1. The serum of the normal individual (peaks [4] and [5]) barely show the MPS-1 peaks. Proteins denoted [1, 2 and 3] are serum carriers for MPS-1 protein in both Figure 3A and B. Proteins [6, 7 and 8], have been previously identified as HPHU-2, HPHU-1, and C3a [Anaphylotoxin] (6). Figure 3C. Peaks [1 to 6] are molecular weight markers.
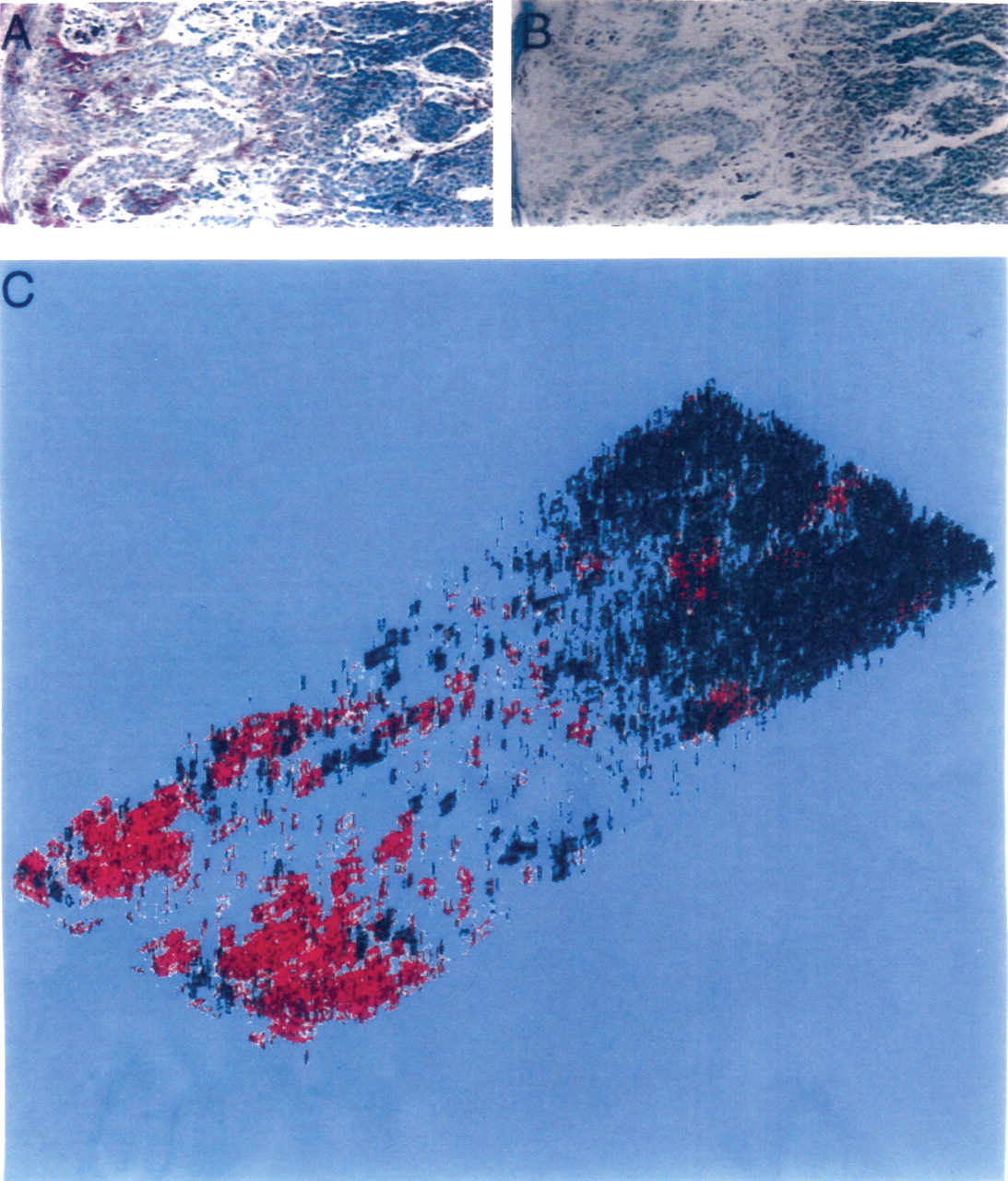
Analysis of superficially spreading malignant melanoma to adjacent tissues indicate induction of apoptosis by melanoma cells which illustrates the origin of MPS-1 in the serum of patients, illustrating the origin of MPS-1 in serum of patients with cancer (Figure 4). Figure 4A, shows melanoma cells stained for MPS-1 (red stain). Figure 4B, corresponds to an adjacent section of Figure 4A, processed to detect apoptosis (brownish/black stain). The brownish/black stain indicates nucleus fragmentation of DNA which shows initiation of apoptosis in the melanoma cells. Figure 4C is a 3D computer tomographic reconstruction, of alternative and adjacent melanoma cells and apoptotic cell tissue sections, with increased levels of MPS-1 (Red stain), and apoptosis of adjacent keratinocytes (Black stain). About one-hundred alternative and consecutive slices were stained for MPS-1 and apoptosis. The sections were alternatively stained with: (i) anti-MPS-1 antibodies (AA 2-17 peptide, and (ii) processed for apoptosis by detecting DNA fragments.
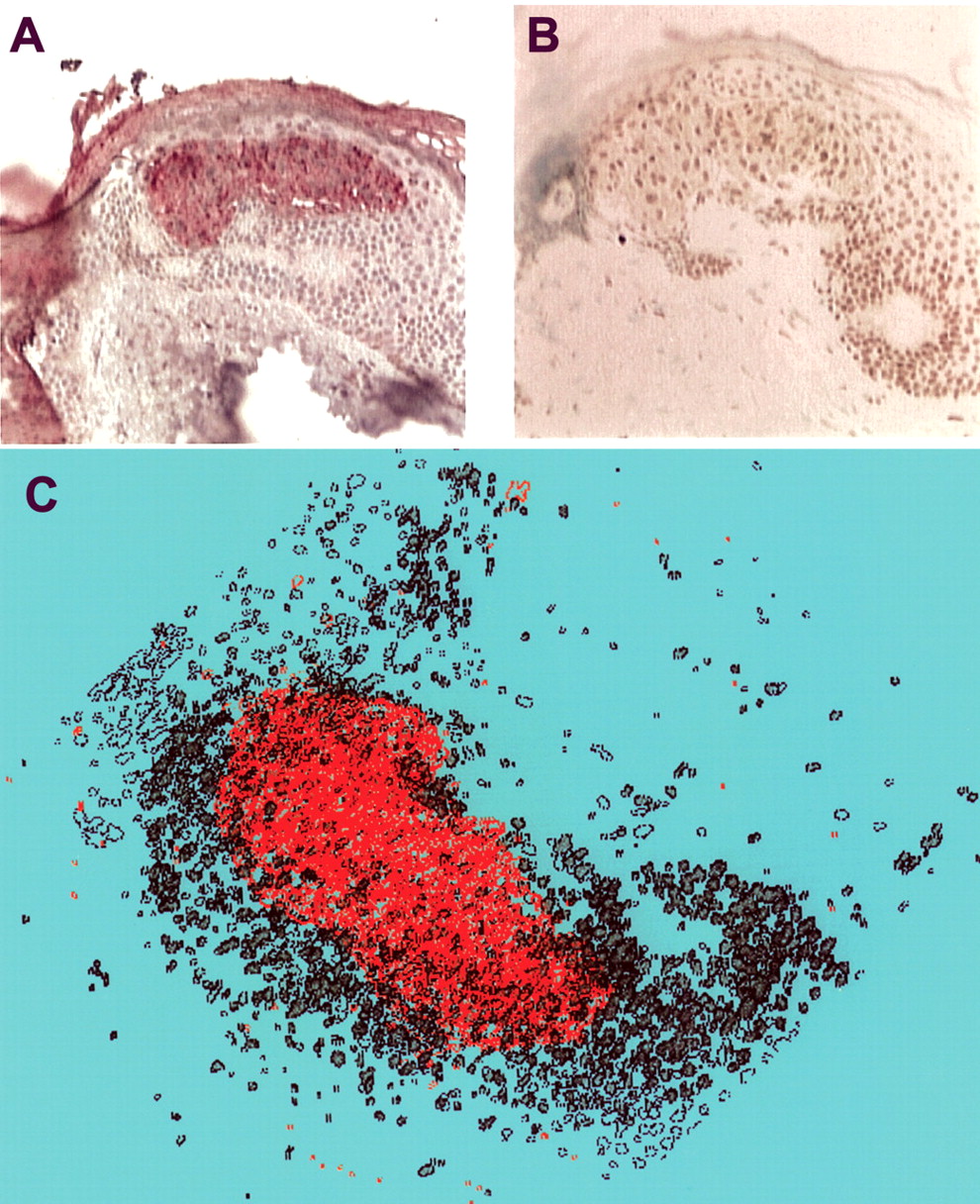
MPS-1 expression and apoptosis in benign nevi. Figure 5A shows the MPS-1 staining pattern in benign nevi, which shows intensely positive superficial type A melanocytes (24). The apoptosis staining pattern (Figure 5B) is observed as a gradient, opposite to the MPS-1 gradient, from intensely positive in deep areas of the skin to negative in surface areas. Figure 5C is a 3D tomographic reconstruction of tissue slices corresponding to slices alternatively stained for MPS-1 (red stain) and apoptosis (B, black stain), which is in a gradient from intensely positive superficial type A melanocytes (MPS-1, red stain) to negative type C (black, apoptosis).

MPS-1 is expressed in placenta and released into the blood by the invasion of the uterine wall by syncitiotrophoblasts cells during healthy pregnancy in a time-dependent fashion. (A) histochemistry of placental cells labeled with anti-MPS-1 antibodies; (B) MPS-1 neutralized with MPS-1 peptide 2-17 which prevents staining, showing specificity; (C) bottom, five separate healthy pregnant women progressively increased the MPS-1 level in the 1st, 2nd and 3rd trimester of pregnancy.

MPS-1 identified by immunoblot studies in sera of cancer patients with anti-MPS-1 antibodies (AA 2-17); (A) the serum was obtained from a patient with metastatic cancer. Peaks 4 and 5 correspond to MPS-1 (4 is the major peak of 9.8 kDa; a degradation product of MPS-1 is also detected, Peak 5). As can be seen the serum of a normal subject (B), peaks 4 and 5) barely shows the MPS peaks. Proteins denoted 1, 2 and 3 are serum carriers for MPS-1 proteins in both A and B. Proteins 6, 7 and 8 have been previously identified as HPHU-2, HPHU-1, and C3a [Anaphylotoxin] (Ref. 6). (C) Peaks 1 to 6 are molecular weight markers. Note the very low levels of MPS-1 in B, normal serum.
Measurement of MPS-1 in serum of healthy individuals and in patients with different types of malignant and benign tumors. In a series of experiments with about 1200 patients, the data showed the general distribution of MPS-1 values for active cases of cancer disease (clinical evidence of disease progression). Initially we found that 85% of the patients in this group showed MPS-1 levels in the range of 20 to >50 ng/mL. In 9% of the individuals in this group, the MPS-1 levels ranged from 10.01 to 20 ng/mL (intermediate “grey area”). Thus, elevated MPS-1 levels identified patients with active malignant tumors with at least 80% confidence limits (14-17). It is interesting to note here that in patients with metastatic cancer of various origins, such as prostate and colon, the MPS-1 levels were in most instances (>75% of the cases) extremely high (100 to 1000 ng/mL). Non-malignant diseases: The combined results for all nonmalignant diseases (e.g. liver cirrhosis, hepatitis C) indicate that 75% of the patients in this group had MPS-1 levels of <10 ng/mL. In 21% of the individuals in this group MPS-1 levels were in the area of 10.01 to 20 ng/mL (intermediate grey area). Only 1% of the patients with numerous other nonmalignant diseases (N=201) had MPS-1 levels of about 20 ng/mL or lower (N=2).
MPS-1 in sera of patients evaluated for cancer. Table II shows the measurement of circulating MPS-1 in sera of patients evaluated for cancer. In this series 1245 patients were tested. The results of studies with healthy individuals indicate a MPS-1 reference range for adults (Table II; 19-88 years) of non-detectable to 10 ng/mL (82% of the healthy population). In 17% of the individuals in this group MPS-1 levels were in the range of 10.01-20 ng/mL, denoted the gray area, because of the significant overlapping with both active cancerous disease and non-malignant conditions at this range level. In the following Tables (III, IV, V, VI, VII, VIII, IX, X, XI, XII, XIII and XIV) the patients shown are divided by type of tumor. Table II was used to initially divide the MPS-1 range of values as follows: <10 ng/mL; 10-20 ng/mL, and 20 to 30 ng/m. In patients with metastatic cancer of various origins (e.g. prostate, lung, melanoma, etc.), the MPS-1 levels were in most instances (>70% of the cases) extremely high (100 to 1000 ng/mL). Table II also illustrates patients with prostate cancer stage M1b (metastasis to the bone) that showed the highest levels observed in this study.

Analysis of superficially spreading malignant melanoma to adjacent tissues indicate induction of apoptosis. A shows melanoma cells stained for MPS-1(red stain); B corresponds to an adjacent section of A processed to detect apoptosis (brownish/black stain). As can be observed, the dark nucleus indicates fragmentation of DNA which indicates initiation of apoptosis in the melanoma cells; C represents a 3-D computer reconstruction of melanoma cells with increased levels of MPS-1 (Red stain) which are aggressively phagocytizing adjacent melanoma cells, and also inducing apoptosis of adjacent keratinocytes (black stain). About 100 slices of a skin melanoma sample, superficially spreading, were sectioned and alternatively stained with (i) anti-MPS-1 antibodies (Red stain) and; (ii) processed for detection of apoptosis (black stain) which was detected by staining DNA fragments. Figure 4A shows staining with anti-MPS-1 antibodies and Figure 4B shows the apoptotic nuclei of keratinocytes surrounding melanoma cells. Figure 4C shows the 3-D reconstruction of this specimen. It was carried out by using a Jurassic Park Silicon Valley Computer.

MPS-1 expression and apoptosis in benign nevi. A: MPS-1 staining pattern of benign nevi is in a gradient from intensely positive superficial type A melanocytes (MPS-1, red stain) to negative type C (black staining, apoptosis). B: The corresponding apoptosis staining pattern is present as a gradient opposite to the MPS-1 gradient, from intensely positive in deep areas of the skin to essentially negative in surface areas. C: Reconstruction of the 3D structure was done utilizing the Jurassic Park Silicon Valley Computer.
Measurement of circulating MPS in sera of patients with nonmalignant diseases.
Measurement of circulating MPS in sera of patients evaluated for BPH.
Measurement of circulating MPS in sera of patients evaluated for prostate cancer.
Further analysis of the sub-groups with non-malignant diseases revealed that only 1% of the patients with numerous other non-malignant diseases (N=201) had MPS-1 levels > 20 ng/mL. Table II was divided according to type of cancer and analyzed in the following Tables (III, IV, V, VI, VII, VIII, IX, X, XI, XII, XIII and XIV).
Measurement of circulating MPS-1 in serum of patients with non-malignant diseases (Table III). The number of patients studied in this group was 197. The combined results for all non-malignant diseases listed in Table III indicate that 75% of the patients in this group had MPS-1 levels <10 ng/mL. Less than 4% of the patients with these conditions had MPS-1 levels >10-15 ng/mL and, only 12 patients had levels >15-20 ng/mL.
Measurements of circulating MPS-1 in serum of patients evaluated for benign prostatic hypertrophy (BPH) (Table IV). The number of patients with BPH studied was 48. The BPH untreated patients were plotted at the bottom of Table IV to facilitate comparisons. Individuals with untreated BPH (left chart) and treated BPH (right chart) are shown in graph form at the bottom of Table IV. BPH untreated patients had levels from 2 ng/mL to 50 ng/mL MPS-1. After treatment, 11 patients showed a decrease in MPS-1 from 2 ng/mL to 15 ng/mL. The BPH patients not shown in the graphs were treated by non-surgical means. Thus, MPS-1 is a useful marker to determine removal of BPH tissue from the prostate grand.
Measurements of circulating MPS-1 in serum of patients evaluated for prostate cancer (Table V). A group of 177 patients with prostate cancer were studied. The following groups are shown in graph form at the top or the bottom of Table V: (i) Prostate cancer untreated patients (top left); (ii) prostate cancer treated patients in remission (P-RM) (top right); (iii) Untreated metastatic prostate (bottom left); and (iv) treated metastatic prostate cancer in remission (M1b-RM) (bottom right). Note the large decrease in MPS-1 in both prostate cancer and M1b metastatic prostate cancer in P-RM) after treatment of patients. For example, the M1b metastatic prostate cancer in 10 patients showed MPS-1 levels reduced from 2 to 8 ng/mL.
Measurements of circulating MPS-1 in sera of patients evaluated for colorectal cancer (Table VI). The following groups are shown in graph form at the top or bottom of Table VI: (i) Colorectal cancer untreated patients are shown at the top left; (ii) colorectal cancer treated patients in RM (C-RM) are shown at the top right; (iii) untreated metastatic colorectal cancer (C) is shown at the bottom left; (iv) metastatic C-RM (5 patients), and metastatic colon-prostate cancer in RM (2 patients) are shown at the bottom right. The distribution of MPS-1 values for colorectal carcinoma and premalignant polyps are shown in Table VI. Active cancer and cancer in remission are shown for stages T1-T4 and for Metastatic M1a.b.c. Active colon CA showed levels >20 ng/mL which, after treatment and RM, were decreased significantly. The bottom two figures show active C-CA (left) and RM of colon cancer (right).
Measurement of Circulating MPS in sera of patients evaluated for colorectal cancer.
MPS in sera of patients evaluated for hormones
MPS-1 in serum of patients evaluated for various hormones (Table VII). Human growth hormone showed one out of 6 values for MPS-1 elevated. Insulin-like growth factor 1 showed 2 out of 6 values for MPS-1 elevated. C-term PTH (dialysis patients) showed all MPS-1 values elevated except one. Low PSA levels corresponded well with low MPS-1 levels except for one patient after surgery (38.7 ng/mL) for MPS-1. Primary hepatocellular carcinoma showed MPS-1 elevated to high levels in 5 out of 6 patients. Prostatic carcinoma showed 10 patients with MPS-1 elevated levels out of 14 separate patients. NSE: Neuroendocrine cell tumors (six patients) all showed very high levels of MPS-1. Gastric carcinoma (CA 72-4) showed all 6 patients with highly elevated MPS-1. Four out of 6 samples of patients with breast cancer (assay CA 15-3) showed 4 samples with elevated MPS-1. Pancreatic carcinoma (assay CA 19-9) showed that the MPS-1 was greatly elevated in all samples. CEA showed 6 out of 8 samples with greatly elevated MPS-1 levels. Ovarian cancer (assay CA 125) showed 4 out of 5 samples with elevated MPS-1 levels. The values for normal females and males are also shown in this Table. As previously shown, MPS-1 levels are elevated in healthy pregnancy.
A. Measurement of circulating MPS in sera of patients evaluated for lung cancer. B. Distribution of MPS values.
Measurement of MPS-1 in serum of patients evaluated for lung cancer (Table VIII-A). The following groups are shown in graph form: (i) lung cancer untreated patients (left) show MPS-1 levels >20 ng/mL in 9 patients and in 3 patients the levels were higher than 10 ng/mL. Thus, all lung cancer patients were positive for MPS-1. Metastatic lung cancer shows very high levels of MPS-1 (from 200 to 450 ng/mL). Table VIII-B shows the distribution of values for lung cancer: (i) Primary lung cancer showed 25 to 50 ng/mL of MPS-1; (ii) primary metastatic lung cancer levels of MPS-1 were 100 ng/mL; (iii) primary lung and prostate cancer in the same patients, showed MPS-1 levels of 66.6 and 33.3 ng/mL; (iv) primary lung and prostate, stage M1,a,b,c levels were >100 ng/mL; and (iv) secondary metastatic to the lungs showed MPS-1 levels of 20.1 to 50 and >50 ng/mL. The graphic distribution of MPS-1 values for lung cancer are shown at the bottom of Table VIII-B and correspond to categories 3, 4, and 5 (10, 20, and >50 ng/mL).
Table IX illustrates measurements of MPS-1 in serum of patients evaluated for head and neck tumors which were then plotted to compare healthy individuals with untreated patients having squamous cell carcinoma (SSC). The MPS-1 values shown in Table IX correspond to untreated patients with SCC. As can be seen the elevated levels of MPS-1 in SCC are useful to detect SCC patients, confirming previous results (18-19).
Table X shows the levels of MPS-1 and CA-15-3 in the same serum specimens of breast cancer patients in different clinical stages, and correlate these serum values with cancer stages. The levels of both MPS-1 and CA-15-3 were plotted to investigate the correlation of cancer stages with tumor marker levels.
The plotting of MPS-1 values in untreated breast cancer patients corresponding to Table X, which are organized in ascending MPS-1 concentrations, show the striking importance of the MPS-1 test for early detection of breast cancer and its correlation with clinical stages. The individual values plotted for each marker correspond to tumor marker measurements done in the same samples. In the plotting, the vertical lines separate from left to right breast cancer stages 0, I, II, III, and IV. Stage 0 (T0) indicates non-invasive carcinoma in situ and Paget's disease of the nipple. Stage (I1), tumors of <2 cm. Stage II (T2) tumors from >2 cm to <5 cm. Stage III (T3), tumor of >5 cm. Stage IV (M), distant metastasis present.
The breast cancer tumor marker/stage plotting, obtained from Table X, shows a study which includes 200 patients ranging from T0 to Stage IV (M). The comparison of MPS-1 with the routine tumor markers CA 15-3 and CEA are also shown. CA-15-3 and CEA values were of little or no clinical use to correlate with breast cancer stages. It is undeniable that the use of MPS-1, is far superior for the detection of early breast cancer than CA-15-3 or CEA, which were ineffective.
Head and neck tumors.
Table XI shows 30 separate healthy female serum specimens, in which the MPS-1 was measured. As can be noted, from 29 normal samples 28 were in the normal range of about 10 ng/mL, while only one sample (No. 13) showed levels of 15 ng/mL indicating that it was in the gray zone of the MPS-1 test, and thus indicated that the assay should be repeated in 3 months. Overall 99% ±2 SD of the MPS-1 values were either about 10 ng/mL ±2 SD or were below that level. Thus, the MPS-1 test is highly reliable in determining the individuals who are highly unlikely to develop a carcinogenic process. The bar graph shows the healthy female MPS-1 serum levels for comparison (values obtained from Table IX). Table XII was used to generate the graphs. Table XII (breast normal values), consisting of 120 patient samples is shown for comparison. The plotting of the 120 samples of MPS-1, CA 15-3 and CEA is also shown (Table XII). The markers are also shown in 120 separate determinations at the bottom of Table XII-breast normal values for MPS-1, CA 15-3 and CEA, indicating further the validity of the MPS-1 serum test for the detection of breast cancer.
Table XIII compares early breast cancer stages 0, I and II with normal female serum from healthy individuals. The age, stage, CEA, CA 15-3 and two separate measurements of MPS-1, E1 and E2, in two separate MPS-1 assays are shown to determine the inter-assay coefficient of variation (14). The findings indicate that stages 0, I and II can be detected early by the MPS-1 test in >90% of the cases, confirming previous results presented above.
Table XIV shows comprehensive and detailed data on a large number of patients with advanced breast cancer (stages III and IV). A few early cancers are also included in this series (stages I and II). Table XIX shows stage I (8 patients), stage II (5 patients), stage III (9 patients), stage III/IV (5 patients), and stage IV (13 patients). Table XIV indicates the response to various types of therapy and status as: (i) stable; (ii) progression; and (iii) response to therapy. The MPS-1 protein was highly increased in all patients in advanced stages, irrespective of response to therapy, except in four patients.
Discussion
MPS-1 as a “universal or broad spectrum tumor marker is defined as an antigen found in abnormal concentrations in the blood of a large number of patients (>90%) suffering from various forms of benign and malignant neoplastic processes (20-23). The results presented in this article demonstrate that the MPS-1 antigen is a ubiquitous tumor marker that may be useful in early detection, prognosis and management of various types of benign and malignant tumors.
The syncytiotrophoblasts are multinucleated cells present in the placenta of embryos (Figure 2A). The outer syncytial layer of the trophoblasts actively invades the uterine wall. It forms the outer fetal component of the placenta and massively increases the surface area available for nutrient exchange between the mother and the fetus. The syncytiotrophoblast cells secrete human chorionic gonadotropin (hCG). Figure 2C (bottom) shows that the pregnant women studied secrete MPS-1 into the blood during the first, second and third trimester of pregnancy and the levels progressively increase in a time dependent fashion. Figure 2A shows the syncytiotrophoblasts from which the MPS-1 is released into the mother's circulation. These results suggest that MPS-1 may have a role in invasion of normal tissues in oncogenic processes.
Comparison of MPS-1 with the routine tumor markers CA 15-3, CEA and breast cancer stage.
A preliminary attempt determined the ratio of MPS-1 to apoptosis to be greater in melanoma than in basal cell carcinoma and benign nevus (Figure 5) (23). Interestingly, the distribution is different. While in melanoma MPS-1 was easily detected in serum, the benign nevi showed no traces of MPS-1.
It can be suggested that the rapid growth of melanomas in a disorderly fashion and its high phagocytic capacity are reflected by the MPS-1/apoptosis ratios, in which a large proportion of MPS-1 is released in the circulation by apoptosis and phagocytosis by melanoma cells of surrounding keratinocytes (Figure 4A, B and C). In contrast, the MPS-1 staining pattern of benign nevi is in an orderly gradient as clearly shown in Figure 5 A, B and C. The corresponding apoptosis staining pattern in the same benign nevi is also present in a gradient but in a vectorial opposite direction to the MPS-1 gradient, as also shown in Figure 5 A, B and C, making it not possible for MPS-1 to be released into the circulation. Three dimensional tomographic reconstruction of tissue slices corresponding to benign nevi tissues (Figure 5 A, B and C), alternatively stained for MPS-1 and apoptosis shows an orderly pattern (Figure 5C).
Breast cancer is an increasing medical problem, as demonstrated by its high incidence in numerous countries around the world (24-26). In the USA, breast cancer is the most common female neoplasm and the second most common cause of cancer death. Breast cancer research has focused on methods to detect breast cancer at its earlier stages, to cure the disease after early diagnosis. At present, imaging techniques that exploit the different physical properties of the cancer and normal or non-malignant surrounding tissues are used in the early detection of breast cancer. Imaging is also being used as a guide for biopsy. However, the majority of women in the USA (80%), who undergo breast biopsies do not have cancer, indicating the imprecision of imaging techniques (25).
Recognition of the limitations of the latest imaging technologies for early diagnosis of breast cancer and screening of breast cancer has led to the evaluation of new methods of early cancer detection by measuring serum biochemical markers (antigens) released into the blood. More recently the use of proteomic analysis provides unique information which can identify various forms of the same marker (e.g., MPS-1, MPS-like proteins, MPS-1 covalently bound to serum carrier proteins (US Pat. No. 5,955,387) which may be also useful for early detection of breast cancer (7, 11, 13, 24-27). Because of the high incidence of breast cancer even small improvements in early detection and treatment may represent a large number of lives saved or prolonged.
Normal female MPS serum levels.
The experimental tumor marker MPS-1 evolved from cloning of MPS-1 from breast cancer cells and the study of ribosomal proteins (1-9). Since MPS-1 protein is produced by many different types of cancer it is not possible to determine the site of origin or tumor type. However, the presence of elevated levels of MPS-1 clearly indicates that in an otherwise healthy individual carcinogenesis is most likely evolving. Thus, the combination of detection of MPS-1 (AA 2-17 peptide) antigen in the serum at elevated levels follow by diagnostic imaging techniques may provide an economic way of early detection of breast cancer.
Conclusion
The MPS-1 test, which measures a unique serum antigen common to a variety of oncogenic processes, provides the following clinically useful information: (i) First and foremost the MPS-1 test narrows down the uncertainty zone concerning the presence or absence of an oncogenic process; (ii) the MPS-1 test may be useful to signal cases where further clinical investigation of oncogenic processes by a physician is needed; and, (iii) the MPS-1 test is an indicator of potential clinical problems in the area of oncogenesis.
Breast normal values.
Breast cancer MPS levels.
Breast cancer response to therapy.
Future Prospects
The information presented here, with a large panel of benign diseases, a larger panel of early stage cancers, and longitudinal studies provide substantial preliminary evidence about the potential efficacy of the MPS-1 test in the early detection of a broad spectrum of oncogenic processes.
It is worth noting here, that healthy individuals with MPS-1 levels <10 and lower, were free of cancer (>99.0%) by standard imaging methods such as CAT, MRI, or PET. Thus, the likelihood of cancer in subjects with <10 ng/mL of MPS-1 in the serum correlates with the absence of cancer with a correlation coefficient of p<0.001%. Therefore, it is conceivable that the MPS-1 test may be useful to detect numerous types of malignancies in early stages of development, thereby reducing the mortality and morbidity rate from various types of cancers, and thus the enormous expenditures associated with negative imaging diagnosis and various cancer treatments used in advanced cancer. Levels lower than 10 ng/mL appear to indicate in a large series of subjects the absence of any type of carcinogenic process as described in this extensive article with various cancer types.
Quality criteria. As can be calculated from total distribution of MPS-1 values shown in the Tables, the quality criteria of the MPS-1 test as a tumor marker, characterized by its diagnostic specificity, sensitivity, and the cutoff value indicate that the MPS-1 test has high specificity (>75%) and sensitivity (>89%), as a tumor marker. However, the MPS-1 test cannot identify the site of origin of the tumor. Thus, it should be used in combination with other physical techniques such as CAT, MRI, PET. Thus, low levels of MPS-1 (<10 ng/mL) indicate with high probability that the individuals are most likely free of cancer disease, and thus, further screening with CAT, MRI and PET could be avoided.
Acknowledgements
This research was supported by Antagoras AG, LLC., St Louis, MO, USA, designated research funds.
- Received May 7, 2012.
- Revision received June 30, 2012.
- Accepted July 2, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}