


Abstract
The aim of this study was to: To investigate topoisomerase IIα (topo-IIα) expression and its correlation with clinicopathological parameters in primary gastric cancer patients. Patients and Methods: A tissue microarray including tumor, paired non-tumoral and lymph node metastasis specimens from 210 gastric adenocarcinoma patients was built for immunohistochemical interrogation. The correlation between topo-IIα expression and patient clinicopathological parameters was evaluated by univariate and multivariate analyses. Results: High topo-IIα expression was observed in 30.00% (63/210) of the primary tumors, 25.27% (23/91) of the lymph node metastases and 0.47% (1/210) of the non-tumoral gastric mucosa (p<0.001). Topo-IIα expression in the gastric adenocarcinoma was positively correlated with tumor location (gastric cardia, p<0.001), intestinal histological type (p=0.041), late age onset of gastric adenocarcinoma (≥50 years; p=0.002) and male gender (p=0.038). There was no association with other clinicopathological parameters. No correlation was observed between topo-IIα expression and survival. Conclusion: The prognostic value of topo-IIα in gastric adenocarcinoma remains underdetermined.
Gastric carcinoma ranks as the world's second leading cause of cancer mortality despite a sharp worldwide decline in both its incidence and mortality since the second half of the 20th century (1). The currently available first-line treatments for advanced gastric cancer offer a relatively small survival benefit to patients in comparison with the best support care alone (2). The 5-year survival rate for the total population of gastric cancer patients remains less than 25% (3).
The topoisomerase family has been identified as the molecular target of many chemotherapeutic agents. Human cells are known to contain the following five topoisomerase family members: topoisomerase I, IIα and IIβ, IIIα and IIIβ. Topoisomerase II isozymes are the target for the epidophyllotoxins and DNA interacalators such as anthracycline (4). At the present time, anthracycline-based regimens have shown some certain, but limited effects in gastric cancer (5), and they have usually been applied without investigating the status of topoisomerase IIα (topo-IIα). Evaluation of topo-IIα protein expression may be useful in designing rational combination therapies with topoisomerase-targeting drugs. Topo IIα has also been suggested as a cell proliferation marker in both normal and tumor tissues (6) because topo-IIα expression increases during the late S-phase and decreases at the end of the M-phase and anti-topo-IIα antibody labels cells in the S, G2, and M-phases of the cell cycle (7).
Topoisomerase IIα gene (TOP2A) expression has been observed in a variety of tumors, including breast, colorectal, ovarian, hepatecellular and salivary gland carcinomas and topo-IIα overexpression is believed to be associated with aggressive clinical behavior (8-10), which suggested it as a valuable prognostic marker for tumor advancement and recurrence and predictor of poorer survival, as well as its potential use as a clinical target in the treatment of patients (11-16). The immunostaining pattern of topo-IIα in frozen and formalin-fixed, paraffin-embedded human tissue sections has been studied for more than one decade (6-18) and topo-IIα expression in human gastric disorders was first described in 1996 (7), however, a quick survey of the literature has shown that the role of topo-IIα expression as a prognostic marker in gastric cancer remains poorly understood. Several studies have reported topo IIα expression in gastric cancer (7, 12, 19-21), but little was done to analyze the clinical evolution, or relationship with survival in detail.
In the present study, immunohistochemistry (IHC) applied to tissue microarray (TMA) was used to evaluate topo-IIα protein expression in a large, single institution series of 210 gastric adenocarcinoma patients. Further analyses were performed to see if any correlation exists between topo-IIα expression and clinicopathological parameters and survival, in order to assess whether there might be a potential place for topo-IIα as a prognostic factor in this malignancy.
Patients and Methods
Patients. Between 1991 and 2003, patients who underwent gastrectomy for gastric adenocarcinoma in PLA General Hospital were considered candidates for this study. The inclusion criteria of patients were: males or females 20 years of age or older; newly diagnosed (incident) gastric adenocarcinoma without previous treatment; diagnosis histologically confirmed; paraffin-embedded tumor, paired surrounding non-tumoral gastric mucosa tissues available, with carcinomas metastatic to lymph node if possible and positive follow-up results at the time of TMA construction. As a result, 210 gastric adenocarcinoma cases were collected, comprising 173 men and 37 women (27-92 years, mean=59.28 years). Among them, 91 cases had carcinomas accompanied by lymph node metastasis.
Demographic, lifestyle and clinicopathological data for the sample cases are shown in Table I. The follow-up assessed their current status in 2005 by consulting their case documents or through phone calls to patients (or their family members, or family practitioners). A minimum interval of 18 months was adopted, and the median follow-up time for patients who were alive at the end of follow-up was 54 months (range 18 to 153 months). Survival time was calculated from the date of surgery to the date of death or the date last known alive.
Informed consent was obtained from the patients. The Ethical Committee of the PLA General Hospital permitted the use of the tissues and the data for this project.
Preparation of tumor tissue microarrays. All the tissues were fixed in 4% neutralised formaldehyde, embedded in paraffin. Blocks of paraffin-embedded donor tissue were sampled using a Manual Tissue Arrayer 1 instrument (Beecher Instruments, Silver Spring, MA, USA). Two cores were cut from each donor block for the TMA blocks. Sections (5 μm) of the tissue array (`recipient') block were cut and placed on polylysine-coated glass slides and processed for IHC. From the samples available, seven tissue array blocks were prepared, each containing 30 cases with tumor, normal and lymph node tissues if available.
Topo-IIα immunohistochemical staining and assessment. The TMA slides were deparaffinized in xylene and gradient ethanol. Antigen retrieval was performed by placing the slides in a high-pressure cooker in a 0.01 mM citrate buffer, pH 6.0, for 2.5 min at 100°C; they were then cooled for 20 min. Endogenous peroxidase activity was blocked by incubating the section in 3% H2O2 for 10 min, followed by rinsing in PBS solution three times. Immunohistochemical staining was performed with a two-step EnVision(tm)+ System Kit (Dako, Denmark). The sections were incubated with mouse anti-topoisomerase IIα monoclonal primary antibodies (Zymed Laboratories Inc./Invitrogen Corp., San Francisco, CA, USA) at a dilution of 1:35 at 37°C for 60 min, followed by dextran polymer conjugated with horseradish peroxidase enzyme and secondary anti-mouse antibody (Dako). The slides were stained with 3,3'-diaminobenzidine tetrahydrochloride (DAB) chromogen and counter-stained with hematoxylin. A PBS-only staining sample was used as the negative control. Positive controls for topo-IIα were represented by sections taken from breast cancer.
Clinicopathological parameters of gastric adenocarcinoma patients studied in tissue microarray.

Immunohistochemical analysis of topo-IIα expression in (A) primary intestinal type gastric adenocarcinoma; (B) diffuse type gastric carcinoma; (C) tumor metastatic to lymph node; and (D) non-tumoral gastric mucosa. Diffused and strong brownish-yellow nuclear staining of topo-IIα (overall score ≥4) is shown in the intestinal type carcinoma and tumor metastatic to lymph node. Magnification: ×200.
Specific immunostaining for topo-IIα was exclusively confined to the nuclei. It was scored independently and in a blinded manner by two investigators (GJ and WG). Two scores were assigned to each core: the nuclear staining intensity (categorized as 0 [absent], 1 [weak], 2 [moderate], or 3 [strong]) and the percentage of positively stained epithelial cells (scored as 0 [0% positive], 1 [1-25%], 2 [26-50%], 3 [51-75%], or 4 [>75%]). A combined score (overall score) based on the staining intensity and the percentage of cells stained was used to assign a final immunoreactive score. By multiplying the intensity and positivity scores, an overall score of 0-12 was obtained. Topo-IIα staining intensity of 2 and above in at least 25% of the nuclei of the carcinoma cells (overall score of ≥4) was deemed topo-IIα high expression, whereas samples of 3 or less were considered to have low expression.
Statistical analysis. Chi-square test and fisher's exact probability were used to determine the difference in distribution of topo-IIα expression among the categorical variables. Overall survival was examined by topo-IIα expression with Kaplan-Meier curves and analyzed statistically with proportional hazards regression models adjusted for lifestyle and tumor characteristics as covariates. All the p-values were two-sided and considered statistically significant if p<0.05. All the analyses were performed using SPSS 13.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
Topo-IIα expression patterns in normal gastric epithelium and gastric adenocarcinoma. Distinct topo-IIα protein stainings were observed in the primary gastric tumors and lymph node metastasis tumors compared to adjacent non-tumoral gastric mucosa (Figure 1). One hundred and sixty-two out of the 210 non-tumoral gastric mucosa samples showed topo-IIα immunoreactivity, which was located in the nuclei of the cells at the neck of foveolar glands. The median percentage of stained cells was 1% (0-25%). Two hundred and five out of the 210 primary gastric adenocarcinomas and 89 out of the 91 tumors metastatic to lymph nodes showed topo-IIα immunoreactivity, which was located in the nuclei of the carcinoma cells. The median percentage of stained cells was 15% (0-90%) in the primary gastric adeno-carcinomas, and 12% (0-78%) in the lymph node metastatic tumors. Based on the scoring criteria for topo-IIα expression in this study, only one normal tissue sample had high expression, while 63 primary adenocarcinomas had high expression and 23 lymphode metastatic tissue samples had high expression (Table II).

Correlation of topo-IIα expression with clinicopathological features. Primary tumor tissue microarray analysis indicated high topo-IIα expression associated with (A) gastric cardiac adenocarcinoma, *p<0.001; (B) intestinal type, **p=0.041; (C) late age onset of gastric adenocarcinoma, ***p=0.002; and (D) male gender, ****p=0.038.
Topo-IIα expression in gastric tissue samples.
Association between topo-IIα expression and clinico-pathological parameters. High topo-IIα immunostaining score in the primary gastric adenocarcinoma was positively correlated with cardiac gastric adenocarcinoma (p<0.001), intestinal histological type (p=0.041), late age onset (≥50 years; p=0.002) and male gender (p=0.038) (Figure 2), but was not found to be associated with the other clinicopathological parameters listed in Table I (p>0.05). In the 91 patients with both primary tumor and lymph node metastatic tumor specimens, topo-IIα was high-expressed in 23 lymph node metastasis specimens and 25 primary tumor specimens (27.47% vs. 25.27%), which indicated that topo-IIα expression in lymph node metastatic tumor was concordant with topo-IIα expression in primary gastric adenocarcinoma. The topo-IIα expression in the lymph node metastases was not associated with the clinicopathological parameters (p>0.05).
Relationship of lifestyle, tumor characteristics and topo-IIα expression to survival. Follow-up information was available on 204 gastric carcinoma patients for periods ranging from 18 months to 14 years. Overall survival rates were 90.78% (1 year), 79.61% (2 years), 57.77% (3 years), 42.23% (4 years) and 25.73% (5 years), with a median survival of 43 months.

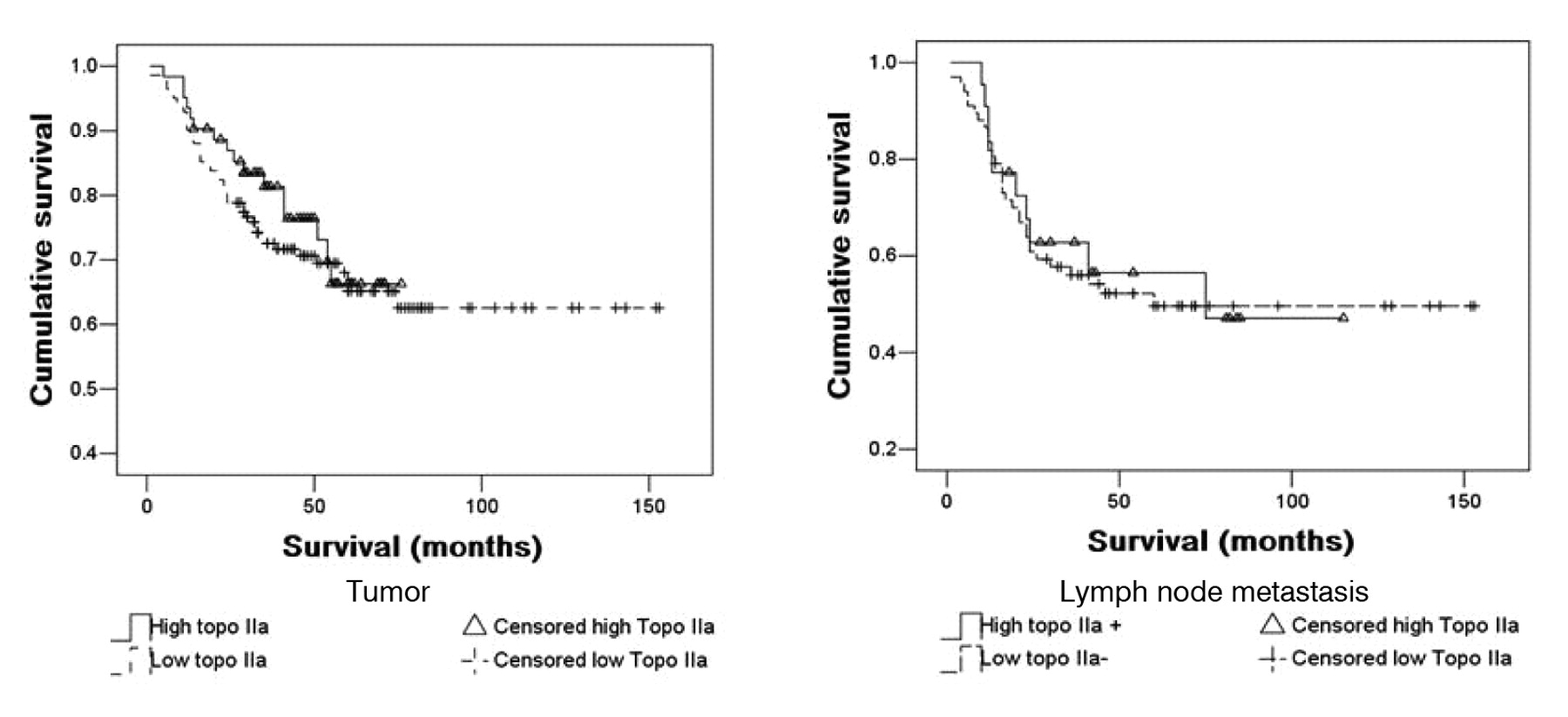
A: Kaplan-Meier curves for 204 patients with gastric adenocarcinoma. Low topo-IIα expression category (142 patients), high topo-IIα expression category (62 patients). No significant difference was observed between the two groups (p=0.555; log-rank test). B: Kaplan-Meier curves of 89 patients with lymph node metastatic tumors. No significant difference in survival between low topo-IIα category (67 patients) compared with the high topo-IIα category (22 patients) (p=0.809).
Adjusted HRs for death by topo-IIα expression in gastric adenocarcinoma patients (n=204).
As depicted in Figure 3, there was no significant difference in survival between patients in the topo-IIα high expression category compared with the low expression category. Univariate analysis using the Kaplan-Meier method was also used to check any possible significant differences with stratification according to tumor location, histological type, age of onset and gender. No correlation was observed between topo-IIα expression and survival in these subgroups (data not shown).
The relationship of topo-IIα expression in the primary gastric adenocarcinoma to survival adjusted for lifestyle and tumor characteristics is shown in Table III. Covariates with p-values less than 0.25 from univariate analysis were selected for further survival analysis. Although higher tumor stage was significantly associated with death, topo-IIα expression did not help predict survival either alone or adjusted for other explanatory variables in the Cox proportional hazards model.
Discussion
In the limited IHC studies reported, high labeling index of topo-IIα was observed in gastric cancer specimens (22-24). In the present study, visually discernible differences in both intensity (moderate or strong, score ≥2) and percentage stained cells (over 25%, score ≥2) were required for clear-cut positive categorization. Compared to normal gastric mucosa, topo-IIα high expression was predominant in the gastric adenocarcinomas, which corroborated the results of previous studies (21-24). The synchronous expression of topo-IIα in both nodal metastases (27.47%) and their corresponding primary tumors (25.27%) may indicate biological consistency of adenocarcinoma cells in primary tumors and lymph node metastases. As in previous studies (7, 21), in non-tumoral gastric mucosa, topo-IIα immunoreactivity was located in the nuclei of the cells at the neck of foveolar glands, which suggested its role in cell proliferation.
The role of TOP2A as a prognostic factor in gastric cancer is controversial and the sparse results published up till now are contradictory. Some studies have found that topo-IIα was associated with poor differentiation of gastric cancer (12, 20), while in other reports, no significant correlation was observed between topo-IIα positivity and any of the clinicopathological parameters studied, including survival (24, 25). In contrast to its indication of poor prognosis and short tumor survival, Liu et al. reported that improved overall survival was found in patients with TOP2A amplification and topo-IIα overexpression (26). Most of the above studies were performed at the gene level. TOP2A gene amplification and increased protein expression have demonstrated concordance (23, 27). The detection of topo-IIα by IHC at the protein level may help in predicting clinical outcomes in gastric cancer patients. In the present study, a higher rate of topo-IIα expression was noticed in the gastric cardiac than in the non-cardiac (gastric body+antrum) tumors; while a higher rate of topo-IIα expression was observed in the intestinal than in the diffuse type tumors. Furthermore, topo-IIα expression was associated with a late age onset (≥50 years). The expression pattern of topo-IIα in gastric cancer presented here has not been reported in the literature. Interestingly, these expression patterns are similar to those of HER2 protein expression in gastric cancer presented recently (28, 29). TOP2A and HER2 are located adjacent to each other at chromosome band 17q12-q21 (30). This might be the molecular basis of their similar expression patterns in gastric carcinoma.
No prognostic role of topo-IIα was confirmed in this study. Hanahan and Weinberg proposed six essential physiological hallmarks that normal cells must acquire to become carcinogenic, in which the ability to proliferate without exogenous stimulation was listed as the very beginning of the procedure (31). Topo-IIa predominates in proliferating cells, present in the S through G2/M-phases of the cell cycle and declines thereafter. Thus, TOP2A amplification and overexpression is an early step of gastric carcinogenesis, which implies that TOP2A expression might have no difference in specimens from various stages and grades of differentiation.
In conclusion, high topo-IIα expression is common in both primary gastric adenocarcinoma and lymph node metastasis; with correlation between high topo-IIα expression and tumor location (gastric cardia), histological type (intestinal type), gender (male prevalence) and late age onset (≥50 years). The prognostic role of topo-IIα in gastric carcinoma however remains an open question, due to the limited number of patients studied, as well as the limitations of the IHC technique itself.
Disclosure
The Authors to declare have no conflict of interest.
Acknowledgments
This study was funded by grants 30740079 from the National Natural Science Foundation of China.
- Received January 9, 2011.
- Revision received March 14, 2011.
- Accepted March 15, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}
{kind=link}