


Abstract
Background/Aim: The immune system has a pivotal role in modulating the response to chemotherapy in breast cancer (BC). However, the immune status during chemotherapy remains unclear. We evaluated the sequential changes in peripheral systemic immunity markers in BC patients treated with various chemotherapeutic agents. Materials and Methods: We examined the correlation between the peripheral systemic immunity markers, neutrophil-to-lymphocyte ratio (NLR), absolute lymphocyte count (ALC) and the local cytolytic activity (CYT) score obtained by quantitative reverse-transcription polymerase chain reaction of 84 preoperative BC patients. Next, we observed the sequential changes in the peripheral systemic immunity markers during treatment with four anticancer drugs: oral 5-fluorouracil derivative; S-1, epirubicin plus cyclophosphamide; paclitaxel plus the anti-vascular endothelial growth factor antibody bevacizumab, and eribulin in 172 HER2-negative advanced BC patients. Finally, we examined the correlation between the changes in the peripheral systemic immunity markers, time to treatment failure (TTF) and progression-free survival (PFS). Results: A negative correlation was found between ALC and NLR. ALC-low and NLR-high cases were positively associated with CYT score-low cases. The ratio of ALC-increase and NLR-decrease varies depending on the anticancer drugs used. The responder group (TTF ≥3 months) had a higher NLR-decrease ratio than the nonresponder group (TTF <3 months). Patients with a high NLR-decrease ratio showed higher PFS. Conclusion: The change in ALC or NLR varies according to the anticancer drugs, suggesting differential immunomodulatory effects of the drugs. Furthermore, the change in NLR reflects the therapeutic efficacy of chemotherapy in advanced BC.
Breast cancer (BC) is one of the most common female malignancies, seriously affecting people’s quality of life worldwide (1). Thus, it is a major public health problem that remains to be solved.
Recently, the pivotal role of the immune system in modulating tumor progression and the response to various treatments, including chemotherapy, has been recognized (2, 3). Moreover, immunotherapy combined with chemotherapeutic agents has become a mainstream treatment for cancer, including BC (4). Therefore, the therapeutic effect of anticancer treatments, including chemotherapy, may be affected by the patient’s immune status.
Chemotherapy affects various cells, including inflammatory and immune cells. The majority of chemotherapeutic drugs, when used at clinically effective doses, have intrinsic immunosuppressive properties since they preferentially kill rapidly proliferating cells (5). However, several anticancer agents stimulate tumor-specific immune responses either by inducing the immunogenic death of tumor cells or by engaging immune effector mechanisms (5). These findings suggest that anticancer drugs, in particular the combination of chemotherapy and immunotherapy, will have different effects on host immunity and different therapeutic effects. Thus, biomarkers that reflect host immunity in real time would be useful in cancer treatment with chemotherapy in the clinic.
Recently, increasing evidence has shown that peripheral blood cell counts or ratios, such as the absolute lymphocyte count (ALC) and neutrophil-to-lymphocyte ratio (NLR), reflect the general immune status of patients with various malignancies (6-9). Interestingly, not only baseline values but also the changes of ALC and NLR during anticancer treatment are associated with prognosis and/or treatment efficacy in patients with various cancers (10-20). We hypothesized that the sequential dynamics of ALC and NLR reflect the changes of host immune status during the treatment with various anticancer drugs, and that these dynamics could serve as a cost-effective biomarker with easy accessibility to predict the treatment response.
In this study, we observed the sequential changes in ALC and NLR during treatment with four key anticancer drugs that are used in BC worldwide: an oral 5-fluorouracil derivative (S-1), epirubicin plus cyclophosphamide (EC), paclitaxel plus the anti-vascular endothelial growth factor (VEGF) antibody bevacizumab (PB), and eribulin (Eri). Then, we explored the differences in ALC and NLR changes according to the drugs. Furthermore, we examined whether changes in ALC and NLR reflect the therapeutic efficacy of these anticancer therapies.
Materials and Methods
Study patients. We reviewed the medical records of patients with HER2-negative advanced BC who underwent chemotherapy (first to fourth-line) at Kyushu University Beppu Hospital (Oita, Japan) and the Ueo Breast Cancer Hospital (Oita, Japan) (affiliated with Kyushu University Beppu Hospital) between January 2017 and May 2021. Patients were treated with at least one of four therapies: the oral 5-fluorouracil derivative S-1, epirubicin plus cyclophosphamide (EC), paclitaxel plus bevacizumab (PB), or eribulin (Eri). All patients fulfilled the following criteria: 1) histologically confirmed HER2-negative invasive BC, 2) unresectable, metastatic BC, 3) had received at least two cycles of chemotherapy, and 4) Eastern Cooperative Oncology Group Performance Status grade ≤2 and adequate organ and hematological function. We excluded patients who did not undergo imaging tests, such as systemic computed tomography during chemotherapy, and those who had myelocarcinosis. We also excluded patients who received granulocyte colony-stimulating factor (pegfilgrastim).
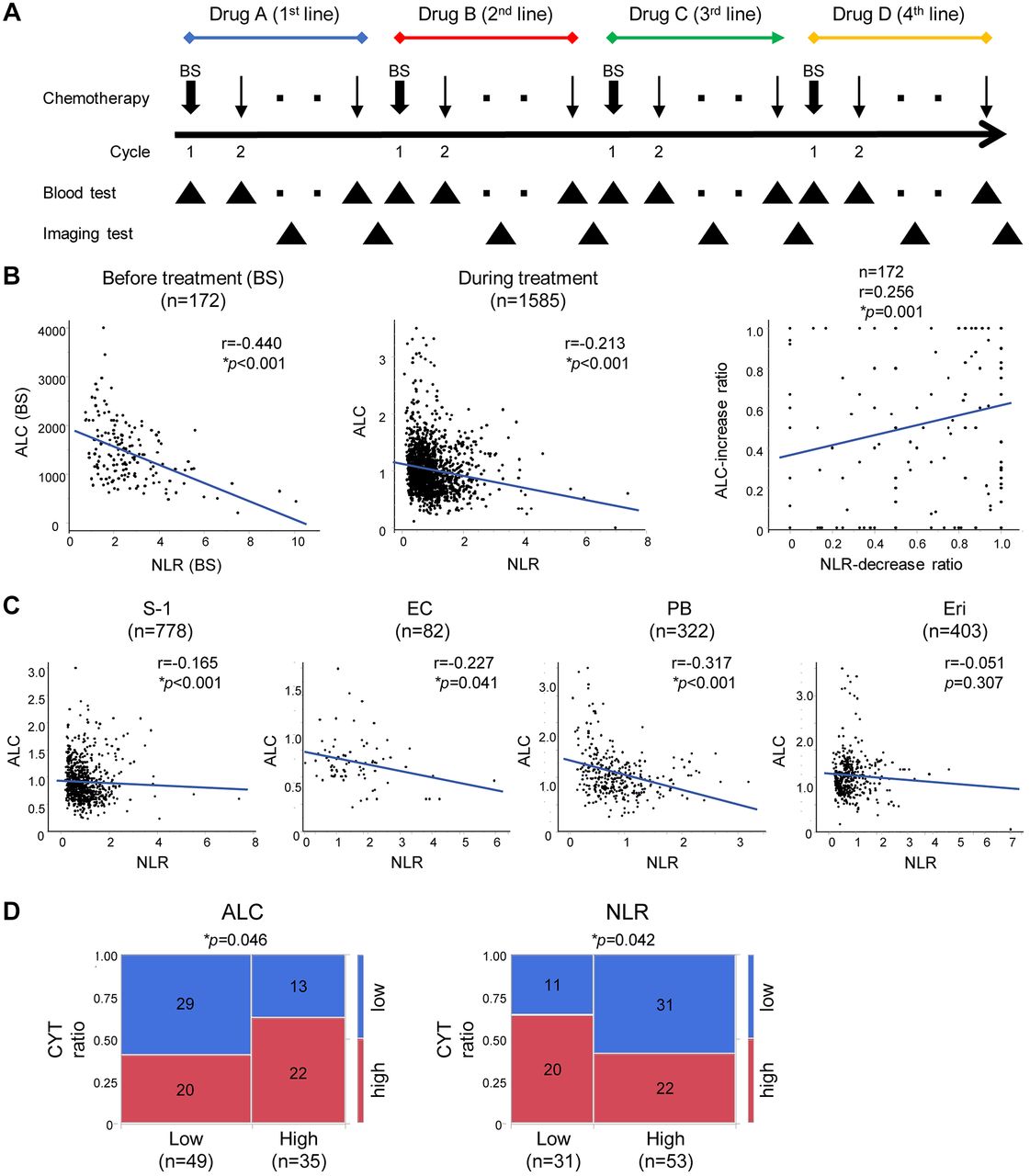
Observation was continued until the patient experienced disease progression, according to imaging test findings, or until the last day when the patient underwent an imaging test, if no disease progression was detected. Disease progression was defined as new metastases and/or growth of pre-existing metastases based on imaging tests such as systemic computed tomography findings. The treatment sampling protocol is shown in Figure 1A. The clinical characteristics of 172 BC patients at the beginning of each chemotherapy are provided in Table I.

Correlation among ALC, NLR and CYT in BC patients. (A) The treatment and sampling protocol. (B) The correlation between ALC and NLR in advanced BC patients. Left, before treatment (n, number of samples); middle, during treatment (n, number of samples); right, the correlation between the ALC-increase ratio and NLR-decrease ratio (n, number of patients). (C) The correlation between ALC and NLR in advanced BC patients according to the anticancer drugs. n, number of samples. (D) The correlation between ALC, NLR and CYT score in BC patients. The cutoff values of ALC, NLR and CYT scores were 1700, 1.75 and 31.56, respectively. n, number of patients. ALC and NLR were expressed relative to the level prior to treatment with each line of therapy (BS=1.0). *p<0.05. ALC, Absolute lymphocyte count; NLR, neutrophil-to-lymphocyte ratio; CYT, cytolytic activity; BC, breast cancer; BS, baseline.
Patient characteristics at the beginning of chemotherapy.
In order to observe the mRNA levels of granzyme A (GZMA) and perforin 1 (PRF1) and the internal control RNA18S5 in BC tissues for the cytolytic activity (CYT) score, we obtained tumor tissues with routine blood data. These data included the count of neutrophils and lymphocytes for the ALC or NLR from BC patients without medical treatment for BC who underwent primary tumor resection at Kyushu University Beppu Hospital (Oita, Japan), from 2016 to 2020. All tumor tissues were freshly frozen and stored at −80°C until RNA extraction. We used 84 samples with high-quality RNA for RT-qPCR analysis.
The expression status of the estrogen receptor (ER), progesterone receptor (PgR), and human epidermal growth factor receptor-2 (HER2) in the tumor tissues were defined according to the American Society of Clinical Oncology/College of American Pathologists guidelines (21, 22). Informed consent was obtained in the form of an opt-out on the website, which was approved by each institutional review board and the Ethics and Indications Committee of Kyushu University (#29-597), in accordance with the Declaration of Helsinki.
Systemic treatments. Chemotherapy regimens were as follows: S-1 (40-60 mg orally twice daily for 4 weeks followed by a 14-day rest period), EC (E: 60 mg/m2 and C: 600 mg/m2 intravenously once every 3 weeks), PB (P: 90 mg/m2 on days 1, 8, and 15 and B: 10 mg/kg on days 1 and 15 of each 28-day cycle) and Eri (1.4 mg/m2 intravenously on days 1 and 8 of each 3-week cycle). Depending on the patient’s condition, the doses were reduced to maintain chemotherapy treatments. Treatment was continued until disease progression based on systemic computed tomography findings, unacceptable toxicity, or patient/physician decision. We defined the time to treatment failure (TTF) as the interval between initiating treatment and disease progression.
Sequential NLR and ALC measurements. NLR was defined as the absolute neutrophil count in the peripheral blood divided by the ALC. To avoid division by zero, we added 40 to the neutrophil count of one patient being treated with Eri when calculating the NLR. ALC and NLR data were obtained at the end of each cycle of chemotherapy. ALC and NLR were expressed relative to the value prior to treatment with each line of therapy [baseline (BS)=1.0]. The ratio describing an increase in ALC (ALC-increase ratio) or a decrease in NLR (NLR-decrease ratio) was defined as following: (number of samples whose values are higher or lower than BS)/(number of total samples per patient). The ALC-increase ratio or NLR-decrease ratio was presented as the mean±standard error of the mean.
Total RNA extraction and reverse transcription-quantitative PCR (RT-qPCR). Total RNA was extracted using the AllPrep DNA/RNA Mini Kit (Qiagen, Germantown, MD, USA) according to the manufacturer’s instructions. RT-qPCR of GZMA, PRF1, and RNA18S5 mRNA levels was performed as described previously (23). In brief, RT was performed using random hexamers and the M-MLV reverse transcriptase (Invitrogen, Carlsbad, CA, USA). qPCR was performed using the LightCycler 480 SYBR Green I Master Mix (Roche, Basel, Switzerland). The raw data were presented as the relative cDNA levels from Human Universal Reference Total RNA (Clontech Laboratories, Palo Alto, CA, USA) and normalized to the level of the internal control gene (RNA18S5). Relative quantification of gene expression was calculated by the 2−ΔΔCt method. The primer sequences used for qPCR were as follows: GZMA: 5′-ATCTGTGCTGGGGCTTTGATT-3′ (sense) and 5′-CTGGTTATTGAGTGAGCCCCA-3′ (antisense); PRF1: 5′-GACGTGACTCCTAAGCCCAC-3′ (sense) and 5′-CCCTCTTGAAGTCAGGGTGC-3′(antisense); RNA18S5, 5′-AGTCCCTGCCCTTTGTACACA-3′ (sense) and reverse 5′-CGATCCGAGGGCCTCACTA-3′(antisense).
CYT score measurement. The CYT score, which was obtained by calculating the geometric mean of GZMA and PRF1 mRNA expression levels in tissue (CYT score=√ GZMA×PRF1), reflects the local immune cytolytic activity and prognostic outcomes of patients in various cancers (24).
Statistical analysis. The degree of linearity was estimated by the Spearman’s rank correlation coefficient (r). The variables were compared using the Mann-Whitney U-test or chi-square test. Survival curves were generated using the Kaplan-Meier method and compared by the log-rank test. A two-sided p<0.05 was deemed statistically significant. Statistical analyses were performed using the JMP Pro 16 software (SAS Institute, Cary, NC, USA).
Results
The correlation between ALC and NLR in advanced BC patients. We examined the correlation between ALC and NLR in all 172 advanced BC patients. Spearman’s rank correlation coefficient demonstrated a negative correlation between ALC and NLR in BC patients before and during chemotherapy (r=−0.440 and −0.213, respectively, p<0.001) (Figure 1B), although the r value was under 0.04, which generally indicates a weak correlation. Moreover, we found a positive correlation between the ALC-increase ratio and the NLR-decrease ratio, which are believed to reflect improved immune status during chemotherapy (r=0.256, p<0.001) (Figure 1B).
Next, we observed the correlation between ALC and NLR in advanced BC patients according to chemotherapy regimen. As shown in Figure 1C, the trends indicated a negative correlation between ALC and NLR for all chemotherapies except Eri. These results suggest a weak negative correlation between ALC and NLR in advanced BC patients with chemotherapy.
The correlation between ALC, NLR and CYT in BC patients. We assessed the correlation between ALC, NLR and the CYT score in 84 samples with high-quality RNA for RT-qPCR analysis from preoperative BC patients without anticancer treatment. The patients were divided into two groups (high or low) according to the ALC, NLR and CYT score values by setting each cutoff value with minimum p-Values. The cutoff values of ALC, NLR and CYT scores were 1700, 1.75 and 31.56, respectively. As expected, ALC-low or NLR-high cases were positively associated with CYT score-low cases (chi-square test, p=0.046 and p=0.042, respectively) (Figure 1D), indicating that the ALC or NLR partially reflect local immune cytolytic activity in BC patients.
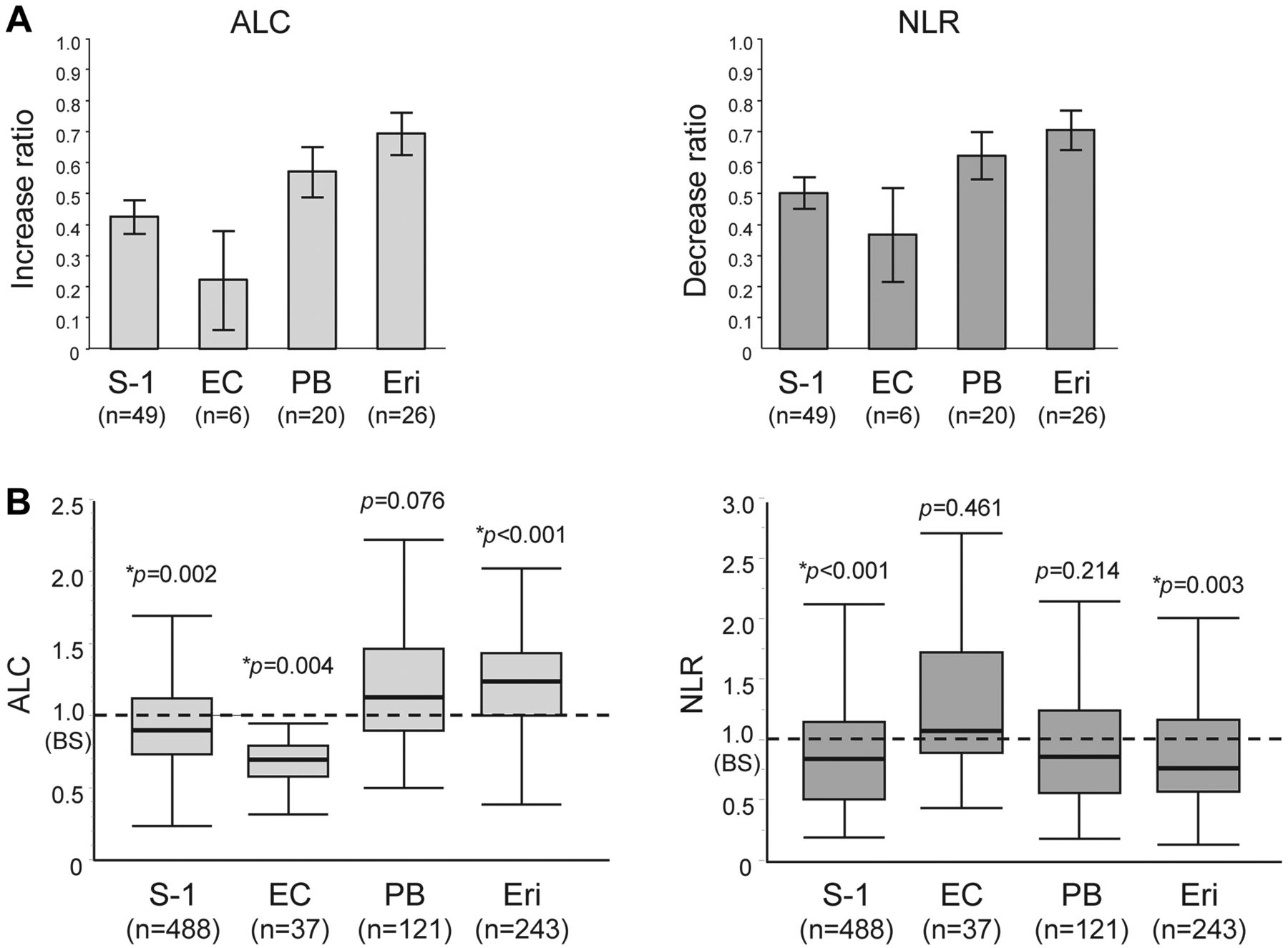
The sequential changes in ALC and NLR during chemotherapy in advanced BC patients. Figure 2A shows the sequential changes in ALC or NLR during chemotherapy with S-1, EC, PB and Eri. An increase in ALC or a decrease in NLR is believed to reflect improved host immunity. As shown in Figure 2B, the ALC-increase ratio or the NLR-decrease ratio varies depending on the anticancer drug in advanced BC patients. This trend was almost consistent with 2 independent cohorts: Ueo and Kyushu datasets. In addition, there was a statistically significant difference in ALC or NLR between before (BS=1.0) and during chemotherapy with each of the drugs (p<0.05, Figure 2C).
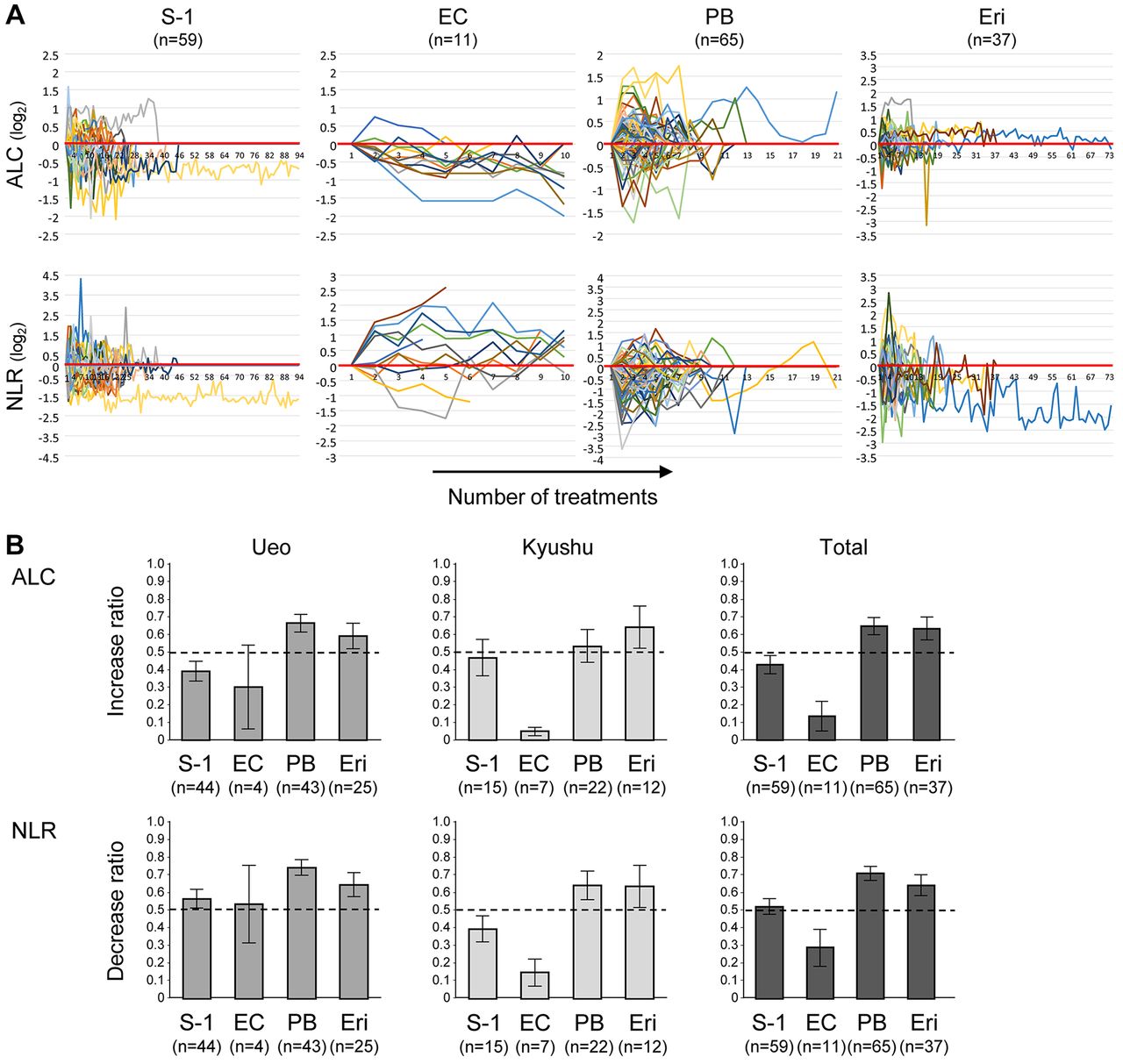

The sequential changes in ALC and NLR during chemotherapy in advanced BC patients. (A) The sequential changes in ALC and NLR during chemotherapy. (B) The ratio of changes in ALC or NLR during chemotherapy according to the hospitals. Left, Ueo; middle, Kyushu; right, total. n, number of patients. (C) ALC or NLR during chemotherapy relative to before chemotherapy. n, number of samples. ALC and NLR were expressed relative to the level prior to treatment with each line of therapy (BS=1.0). *p<0.05. ALC, Absolute lymphocyte count; NLR, neutrophil-to-lymphocyte ratio; BC, breast cancer; EC, epirubicin plus cyclophosphamide; PB, paclitaxel plus bevacizumab; Eri, eribulin; BS, baseline.
These consistent data suggest that the chemotherapeutic drugs may have different immunomodulatory effects. Interestingly, ALC was upregulated while NLR was downregulated by treatment with PB and Eri, providing clinical evidence that PB and Eri can strengthen host immunity.
The sequential changes in ALC and NLR during chemotherapy in advanced BC patients with disease progression. As shown in Table I, therapeutic efficacy varies depending on the drug used. Thus, we observed the sequential change in ALC and NLR during chemotherapy in the 101 advanced BC patients who experienced disease progression. The results of the ratio of ALC-increase or NLR-decrease (Figure 3A) and the difference in ALC or NLR before and during chemotherapy (Figure 3B) were consistent with the above results in all 172 advanced BC patients. These findings reinforce the evidence that the ALC or NLR changes vary depending on the chemotherapeutic drug.
The sequential changes in ALC and NLR during chemotherapy in advanced BC patients with disease progression. (A) The ratio of changes in ALC or NLR during chemotherapy. n, number of patients. (B) ALC or NLR during chemotherapy relative to before chemotherapy. n, number of samples. ALC and NLR were expressed relative to the level prior to treatment with each line of therapy (BS=1.0). *p<0.05. ALC, Absolute lymphocyte count; NLR, neutrophil-to-lymphocyte ratio; BC, breast cancer; EC, epirubicin plus cyclophosphamide; PB, paclitaxel plus bevacizumab; Eri, eribulin; BS, baseline.
The difference in ALC and NLR changes during chemotherapy between front and later treatment lines in advanced BC patients. Figure 4A shows the difference of changes in ALC and NLR during chemotherapy between front (first and second) and later (third and fourth) treatment lines in 172 advanced BC patients. There were no statistical differences between front-line and later lines. Furthermore, the results were the same for all drugs (Figure 4B).

Differences of changes in ALC and NLR during chemotherapy between front and later lines in advanced BC patients. (A) The ratio of change in ALC or NLR during chemotherapy of 172 advanced BC patients. (B) The ratio of change in ALC or NLR during chemotherapy according to the anticancer drugs. Front line, 1st-2nd line; Later line, 3rd-4th line. ALC, Absolute lymphocyte count; NLR, neutrophil-to-lymphocyte ratio; BC, breast cancer; EC, epirubicin plus cyclophosphamide; PB, paclitaxel plus bevacizumab; Eri, eribulin; n, number of patients.
These results imply that the effect on ALC or NLR of each chemotherapy is not significantly changed by the time point of the drug administration, suggesting that chemotherapeutic drugs maintain their immunomodulatory capacity regardless of treatment line.
The difference in ALC and NLR changes during chemotherapy between responders and non-responders to the chemotherapy in advanced BC patients. We compared the therapeutic responses relative to the changes in ALC or NLR during chemotherapy for the 101 advanced BC patients who experienced disease progression. Cases were divided into two groups (responders and non-responders) according to the TTF by setting each cutoff value at 3 months.
As shown in Figure 5A, the trend indicates that the responder group (TTF ≥3 months) had a higher ratio of ALC-increase or NLR-decrease than the non-responder group (TTF <3 months) (p<0.001), although there was no statistically significant difference in the ALC-increase (p=0.276). Also, analysis by the anticancer drugs showed that the responder group (TTF ≥3 months) tended to have a higher ratio of ALC-increase or NLR-decrease than the nonresponder group (TTF <3 months) during chemotherapy, with the exception of patients treated with EC. However, a statistically significant difference was found only in a NLR-decrease for patients treated with S-1 or Eri (p=0.047 and p=0.041, respectively) (Figure 5B). These data indicate that the change in NLR may reflect sensitivity to chemotherapy in advanced BC.

The difference of change in ALC and NLR during chemotherapy between responders and non-responders to chemotherapy in advanced BC patients with disease progression. (A) The ratio of change in ALC or NLR during chemotherapy of 101 advanced BC patients with disease progression. (B) The ratio of change in ALC or NLR during chemotherapy according to the anticancer drugs. Responder, TTF ≥3months; non-responder, TTF <3 months. *p<0.05. ALC, Absolute lymphocyte count; NLR, neutrophil-to-lymphocyte ratio; BC, breast cancer; TTF, time to treatment failure; n, number of patients.
Prognostic significance of the changes in ALC or NLR during chemotherapy of advanced BC patients. We performed a progression-free survival (PFS) analysis of the changes in ALC and NLR during chemotherapy of advanced BC patients. Patients were divided into two groups (high or low) according to the ratio of ALC-increase or NLR-decrease by setting each cutoff value with a BS of 0.5 (baseline).
As shown in Figure 6A, among all 172 advanced BC patients treated with chemotherapy, patients with a high NLR-decrease showed longer PFS compared to patients with a low NLR-decrease (p=0.004). In addition, analysis by the anticancer drugs showed that the low-ALC group during EC treatment and the high-NLR group during S-1 treatment exhibited longer PFS (p=0.002 and p=0.037, respectively) (Figure 6B). Similar to previous reports (19, 25, 26), our results suggest that the change in NLR may affect the therapeutic effect of advanced BC patients during chemotherapy.

Kaplan-Meier PFS curve of advanced BC patients during chemotherapy based on the change in ALC or NLR. (A) PFS is based on the ratio of change in ALC or NLR of 172 BC patients. (B) PFS based on the ratio of change in ALC or NLR according to the anticancer drugs. *p<0.05. PFS, Progression-free survival; BC, breast cancer; ALC, absolute lymphocyte count; NLR, neutrophil-to-lymphocyte ratio; EC, epirubicin plus cyclophosphamide; PB, paclitaxel plus bevacizumab; Eri, eribulin; n, number of patients.
Discussion
In this study, we monitored the sequential changes in ALC and NLR during chemotherapy with four key anticancer drugs, namely S-1, EC, PB and Eri, and showed the differences in their changes according to the drug used to treat HER2-negative advanced BC. Furthermore, we found that NLR changes could be associated with therapeutic efficacy. To the best of our knowledge, this study is the first to evaluate the differences in sequential changes in ALC or NLR during various chemotherapies.
Peripheral systemic immunity markers reflect the general immune status of patients and predict prognosis in various cancers (6-9). However, it was unclear whether ALC and NLR are associated with local immunity. As expected, we found that ALC and NLR are weakly correlated with the CYT score, suggesting that ALC and NLR partially reflect local immunity in BC patients. This finding is supported by several previous studies that showed the NLR or neutrophil count was associated with tumor-infiltrating lymphocytes (16, 27).
In general, chemotherapeutic agents are considered to cause immune cell toxicity followed by immunosuppression (28). However, there is growing evidence that some anticancer drugs can activate host immunity by affecting host immune cells. For example, cyclophosphamide, doxorubicin and epirubicin can kill tumor cells by an immunogenic cell death pathway (29). The immunogenic cell death pathway activates robust innate and adaptive anti-tumor immunity by serving as a therapeutic vaccine and has the potential to greatly increase the efficacy of chemotherapy (4, 30). Gemcitabine and 5-FU effectively deplete myeloid-derived suppressor cells (MDSC) (31, 32), which are innate bone-marrow-derived immune cells that suppress effector T cell responses (33). Cyclophosphamide kills regulatory T cells (Treg), which act to suppress immune responses (34). Notably, we found that the sequential changes in ALC and NLR in advanced BC patients during chemotherapy varies depending on the anticancer drug used. These data provide clinical evidence that anticancer drugs have different immunomodulatory effects, previously uncovered by immunological research (4, 5).
Interestingly, PB and Eri caused an increase in ALC or decrease in NLR regardless of treatment line, providing evidence that PB and Eri could strengthen host immunity. Recently, VEGF was recognized as an important mediator of immune suppression by promotion of Tregs, suppression of dendritic cell maturation, stimulation of tumor-associated macrophages, and infiltration of MDSCs (35, 36), implying that VEGF blockade with bevacizumab may be effective in the antitumor immune response. Eri is considered to have immunomodulatory effects possibly by inducing vascular remodeling followed by reoxygenation and consequent inhibition of the epithelial-to-mesenchymal transition in the tumor microenvironment (37-40). These findings may provide a rationale for using PB and Eri as immunomodulators combined with immunosuppressive anticancer drugs.
Although both ALC and NLR partially reflect local immune cytolytic activity, only the change in NLR was statistically correlated with sensitivity to chemotherapy and PFS in advanced BC. Furthermore, a weak correlation was observed between ALC and NLR of the BC patients treated with chemotherapy compared to those without chemotherapy. The difference between ALC and NLR may be due to the role of neutrophils in malignancies. Accumulating evidence shows that neutrophils participate in tumor growth and metastasis by facilitating tumor cell proliferation ability, invasion potential and angiogenesis by secreting MMP-9 and neutrophil elastase to activate VEGF, inducing neutrophil extracellular traps and suppressing cytotoxic immune cell activity (41). These findings suggest that the cytotoxic effect of anticancer drugs on neutrophils as well as tumor cells may affect the therapeutic efficacy. Further study will be required to clarify this.
A limitation of this study is that it is a retrospective study with a small number of patients. However, despite this limitation, a strength of this study is that it provided detailed observations of data collected during various chemotherapies for advanced BC, supporting the clinical relevance of the changes in host immunity of cancer patients undergoing treatment.
Conclusion
In conclusion, we found that the easy-to-access blood biomarkers NLR and ALC could potentially evaluate immune status in real time during chemotherapy in the clinic. Furthermore, we provide clinical evidence that the immune status of advanced BC patients is affected by anticancer drugs with different immunomodulatory effects. In particular, the dynamic change in NLR could be a useful biomarker to predict patient outcome and response to chemotherapy. Further studies involving a large cohort are required to verify our findings, which could shed light on the host immunity under cancer treatment that may help guide or develop the treatment for cancer patients.
Acknowledgements
We thank Dr. Tyler Lahusen for the helpful comments and English proofreading. We also thank J. Masuda, T. Fukuda, M. Kasagi, S. Sakuma, M. Mishima, and T. Kawano for their excellent technical assistance. This work was supported by the following grants and foundations: Japan Society for the Promotion of Science (JSPS) Grant-in-Aid for Science Research (grant numbers 19K09176, 19H03715, 20H05039, and 20K08930, 20K17556, and 22K09006); OITA Cancer Research Foundation; AMED under Grant Number (22ama221501h0001, 21ck0106690s0201, 20ck0106547h0001 and 20ck0106541h0001); Takeda Science Foundation; The Princess Takamatsu Cancer Research Fund.
Footnotes
Conflicts of Interest
Takaaki Masuda received a donation and research funding from Eisai and LSI Medience, respectively. The other Authors declare that they have no competing interests.
Authors’ Contributions
TM wrote the manuscript. TM and HU conducted the experiments. TM, HU, YO, YK, YA, KM, MK, AK, NH, YT, YH, SS, HO, KF, FT and KM designed the study and interpreted the data. TM prepared the figures and conducted the statistical analysis.
- Received November 24, 2022.
- Revision received December 15, 2022.
- Accepted December 19, 2022.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.