


Abstract
Background: Small cell vaginal carcinoma is a very rare gynecological cancer and treatments including chemo- and radiotherapy have had limited success. Case Report: We report the case of a 37-year-old female, where intensive treatment with the combination of paclitaxel, carboplatin, irinotecan, and camptothecin with and without irradiation did not avoid metastasis of the tumor and the death of the patient. In an attempt to develop a strategy for individualized tumor therapy, we performed immunohistochemistry of 19 cancer-related proteins using a biopsy sample. Strong expression was observed for glutathione S-transferase P1 (GSTP1), epidermal growth factor receptor (EGFR), inducible nitric oxide synthetase (iNOS), nuclear factor kappa B (NF-κB), the oncogene c-MYC, vascular endothelial growth factor (VEGF), and the proliferation marker Ki-67. Intermediate expression was found for the oncogene SRC, β-catenin, and the viral E7 protein. We then performed virtual drug screening with PyRx and molecular docking with AutoDock 4.2.6 by using the three-dimensional structures of these proteins and a chemical library of 1,577 FDA-approved drugs, in a drug repurposing approach. The top 15 compounds were either approved anticancer drugs or drugs used to treat non-malignant diseases. These compounds were bound with comparable or even higher affinity to the targets compared to control inhibitors. Several of these compounds were bound with high affinity to more than one of these target proteins, further supporting the drug repurposing concept. Conclusion: These drugs might offer additional opportunities to reach treatment responses. This approach of individualized tumor therapy might be theoretically not only applicable for small cell vaginal carcinoma but for other tumor entities as well.
Vaginal cancer is a rare gynecologic neoplasm representing only 1-2% of all gynecologic malignancies (1). The vagina is an organ that consists of a fibromuscular tube (7 to 10 cm long) extending from the cervix to the vulva. It is divided into three compartments which are important for classifying tumor location. The lower third is below the level of the bladder base with the urethra anteriorly. The middle third is adjacent to the bladder base, and the upper third is at the level of the vaginal fornices (2). Vaginal cancer is a disease of older postmenopausal women, less than 10% of these tumors occur in patients under 40 years of age. The disease is divided into three types: Squamous cell carcinomas represent more than 90% of vaginal cancer cases, approximately 5% of cases are adenocarcinomas, and small cell carcinoma is very rare (3-5). Squamous cell carcinoma occurs in the proximal third of the vagina, especially the posterior vaginal wall (6). Adenocarcinoma may also arise in the vagina, the majority of which have clear cell histology in young women exposed to diethylstilbestrol in utero (7). The incidence of vaginal adenocarcinoma declined since the routine use of diethylstilbestrol was discontinued in the 1970s.
The vaginal neoplasm is a clinically heterogeneous disease. In young women, the etiology of the disease seems to be related to cervical neoplasia and is, thus, human papillomavirus (HPV)-dependent (8). HPV-negative cancers occur in older women and are often linked to p53 tumor suppressor mutations. The common risk factors for vaginal cancer are tobacco use, sexual intercourse at a younger age, HPV, low socioeconomic status, a history of genital warts, and multiple sexual partners (9). The most common symptoms of vaginal cancer include painless vaginal bleeding and discharge (10). In an advanced stage, urinary retention, pain, hematuria, and frequency of urination may appear (11). Tumors developing on the posterior vaginal wall may produce rectal symptoms, such as tenesmus, constipation, or bloody stool. Early stages of vaginal carcinoma are treated with either surgery or radiotherapy whereas advanced stages are treated with concurrent chemotherapy and radiation therapy.
The vaginal primary small cell carcinoma is rare and represents a highly aggressive malignancy. The survival rate for patients treated in the early stages is around two years (12). The rarity of the disease is considered as the main reason for the uncertainty of the most suited therapy option that is based on the treatment for small cell lung carcinoma (SCLC) (13). Cases of small cell carcinoma restricted to the lung reveal better response rates to chemoradiotherapy compared to chemotherapy alone regarding both complete remission and overall survival (14, 15).
In the present study, we report a 37-year-old patient suffering from small cell carcinoma of the vagina. We describe the clinical course of the disease and the expression profiling as determined by immunohistochemistry. The expression of biomarkers was used to perform a targeted virtual screening of 1,577 drugs approved by the Federal Food and Drug Administration (FDA) in an effort to devise novel treatment strategies for this otherwise hardly curable disease. This concept is based on the idea that drugs approved for one disease might occasionally also exert activity towards another disease (drug repurposing or drug repositioning) and that this approach might be exploited for individualized therapy of cancer patients with otherwise few options by standard chemotherapy and poor survival prognosis.
Patients and Methods
Case presentation. A 37-year-old female from Khartoum, Sudan, was diagnosed in 2015 with small cell carcinoma of the vagina. The patient gave her written informed consent to the present study. The clinical description of the case is based on the clinical documents we have obtained from the patient herself. She sought gynecology service in July 2015 complaining of vaginal discharge, as well as uncomfortable and frequent urination. A mass in the vagina was found during a clinical examination. Histologically, it was diagnosed as poorly differentiated small cell carcinoma. Magnetic resonance imaging (MRI) revealed a tumor of 5×3.9 cm. In September 2015, she started chemotherapy with etoposide and cisplatin for 5 cycles and two further cycles of etoposide and cisplatin in combination with radiotherapy for 32 sessions. In March 2016, MRI performed at the Royal Care International Hospital (Khartoum, Sudan) showed a moderate reduction in the vaginal tumor (4×3 cm) without considerable uptake of contrast agent. There was no evidence of invasion, lymph node involvement, and ascites. In September 2016, the patient suffered severe back and pelvic pain. The MRI investigation of the bone revealed metastases in the L1 vertebra, skull vault, shoulder, and lumber. In October 2016, pain in the lower back region was accompanied by difficulties to walk. A technetium 99m methyl diphosphate bone scan performed at the Royal Care International Hospital (Khartoum, Sudan) revealed increased radiotracer uptake in the skull vault and L1 vertebra indicating bone metastases. The second round of chemotherapy with paclitaxel and carboplatin for 6 cycles was recommended. After three cycles, metabolic activity in the vaginal mass and disturbance in the fat plains between the mass and the bladder wall was found by using positron emission tomography (PET) scan.
The patient suffered from severe back pain, weak urinary stream, and burning micturition. In December 2016, PET/computer tomography (CT) showed metabolic progression of the vaginal tumor, invasion to the bladder wall, and vertebral metastatic deposits. Treatment with radiotherapy, camptothecin, and zoladeronic acid (a bisphosphonate to prevent bone fractures) followed. In January 2017, an MRI diagnosis performed at the Sarvodaya Hospital and Research Center (Ghaziabad, India) showed a lobulated vaginal tumor with central necrosis with a size of 31×25×23 mm and urinary bladder involvement. This hospital treated the patient with paclitaxel and carboplatin combined with fosaprepitant (antiemetic), dexamethasone (anti-inflammatory steroid), palonosetron (against nausea and vomiting) as palliative chemotherapy. The Medanta Mediclinic (New Delhi, India) diagnosed a mild reduction in tumor size (35×10×29 mm versus 41×39×38 mm in the last scan using PET/CT with [18F]-fluorodeoxyglucose (FDG). Back in Sudan in February 2017, the slight regression of the vaginal tumor was confirmed by MRI. Furthermore, a slight regression of the metastases in the L1 vertebra with less surrounding edema was observed (Royal Care International Hospital and a private radiology clinic, Khartoum, Sudan). However, infiltration of the bladder was found by MRI in September 2017. Two cycles of chemotherapy (irinotecan, camptothecin, and zoledronic acid) were applied followed by radiotherapy for 10 sessions.
Afterward, the MRI performed in April 2017 showed that the vaginal mass increased in size with invasion to the bladder wall followed by weak and burning micturition. A PET scan done in September 2017 showed total infiltration of the bladder. Accordingly, the patient was advised to start two cycles of chemotherapy (irinotecan and camptothecin) on a weekly basis and zoledronic acid monthly, followed by 10 sessions of radiotherapy. PET/CT of the vagina obtained in September 24, 2017, revealed a current metabolic and morphological progression. The tumor size was 6.3×5.7×6.5 cm, and the maximum standard uptake value (SUVmax) was 28.9 compared to the previously recorded heterogeneously enhancing vaginal mass (3.5×3.1×2.9 cm, SUVmax: 12.6) (Figure 1A). The tumor mass infiltrated the posterior wall of the urinary bladder (with possible vesicovaginal fistula) and was inseparable from the anterior aspect of the rectum. Metabolic bone progression involved previously noted mild lytic and sclerotic lesions involving the L1 vertebra. A SUVmax value of 12.6 was determined compared to no significant FDG activity (Figure 1B). The patient died on 18 October 2018.

Positron emission tomography/computed tomography scan with 18F-FDG (307 MBq) of (A) the vagina and (B) L1 vertebra.
The paraffin block of the formalin-fixed and paraffin-embedded tumor tissue was obtained from Dr. med. Jalid Sehouli (Charité Universitätsmedizin Berlin, Charité Campus, Virchow-Klinikum, Berlin, Germany).
Immunohistochemistry staining. Antibodies against GSTP1 (rabbit polyclonal, Acris, Herford, Germany, dilution 1:1,000), EGFR (rabbit monoclonal, clone EP38Y, Thermo Fisher Scientific, Dreieich, Germany, dilution 1:500), iNOS (rabbit monoclonal, clone K13-A, Abcam, Berlin, Germany, dilution 1:200), NF-κB p65 (rabbit polyclonal, Thermo Fisher Scientific, dilution 1:200), c-MYC (mouse monoclonal, clone 9E10.3, Thermo Fisher Scientific, dilution 1:200), VEGF (mouse monoclonal, clone VG1, Thermo Scientific Fisher, dilution 1:500), Ki-67 (rabbit monoclonal, clone SP6, Abcam, dilution 1:200), SRC (clone 1F11, Thermo Fisher Scientific, dilution 1:200), β-catenin (rabbit polyclonal, Thermo Fisher Scientific, dilution 1:200), HPV16 E6 (mouse monoclonal, clone C1P5, Thermo Fisher Scientific, dilution 1:500), HPV16 E7 (mouse monoclonal, clone TVG701Y, Thermo Fisher Scientific, dilution 1:500), TCTP (rabbit polyclonal, Thermo Fisher Scientific, dilution 1:200), mTOR (rabbit polyclonal, Thermo Fisher Scientific, dilution 1:200), FTL (clone 8E1E7, Thermo Fisher Scientific, dilution 1:500), CD71 (mouse monoclonal, clone H68.4, Thermo Fisher Scientific, dilution 1:500), ABCB5 (clone 5H3C6, Thermo Fisher Scientific, dilution 1:200), P-glycoprotein (mouse monoclonal, clone C219, Thermo Fisher Scientific, dilution 1:100), BRAF (rabbit polyclonal, Thermo Fisher Scientific, dilution 1:500), and PIK3R (clone U5, Thermo Fisher Scientific, dilution 1:500) were applied on paraffin-embedded tissue slides by using a polymeric labeling technique. Briefly, the slides were washed twice with xylene (98.5% xylene for 5 min each at room temperature) to remove paraffin. Then, the sample tissues were rehydrated through graded washes with isopropanol in water. Heat-induced epitope retrieval was performed using a pressure cooker as a heating device. Ultra-vision protein block and UltraVision Hydrogen Peroxide Block (Thermo Fisher Scientific, Inc.) were added to block endogenous proteins and endogenous peroxidase activity, respectively, to avoid non-specific background staining. Overnight incubation at 4°C was performed following the addition of the antibodies. Subsequently, horseradish peroxidase-labeled polymers conjugated with secondary antibodies specific for both mouse and rabbit primary antibodies were added (Thermo Fisher Scientific, Inc.) at room temperature for 1 h, according to the manufacturer’s protocol. The final staining reaction was performed with diaminobenzidine and slides were counterstained with hematoxylin for 3 min at room temperature.
Immunohistochemistry evaluation. The immunostained slides were scanned by Panoramic Desk (3DHISTECH, Sysmex, Norderstedt, Germany) and evaluated by Panoramic Viewer software (3DHistotech, Sysmex) as previously described (16). Quantification was calculated by dividing the number of positively stained cells by the overall number of cells found in each six independently annotated tumor areas. The mean values of these six areas revealed the average protein expression, while standard deviation values indicated the heterogeneity of expression in the tissue. The higher the standard deviation, the higher was the heterogeneity of the corresponding protein expression in the tumor biopsy.
Virtual drug screening and molecular docking. A total number of 1,577 FDA-approved drugs (17) were subjected to virtual drug screening with PyRx (blind docking mode) (18) for binding to selected target proteins identified by immunohistochemistry. The 3D models of the proteins were obtained from the Protein Data Bank for β-catenin (PDB ID 1JDH), EGFR (PDB ID 1M17), E7 (PDB ID 2B9D), GSTP1 (PDB ID 6Y1E), NF-κB (PDB ID 3GUT), SRC (PDB ID 1YOJ), VEGF (PDB ID 1FLT), iNOS (PDB ID 1NSI). The 15 top-ranked out of 1,577 compounds with the lowest binding energies for the corresponding target proteins were used for molecular docking with AutoDock 4.2.6 (defined docking mode) (19). Three independent docking calculations were performed, each with 2,500,000 energy evaluations and 250 runs by means of the Lamarckian Genetic Algorithm. The corresponding lowest binding energies (LBE) and the predicted inhibition constants (pKi) values were used to calculate mean values±standard deviations. AutoDock Tools and Visual Molecular Dynamics (VMD) were used to visualize the results (Theoretical and Computational Biophysics group at the Beckman Institute, University of Illinois at Urbana-Champaign) (20).
Results
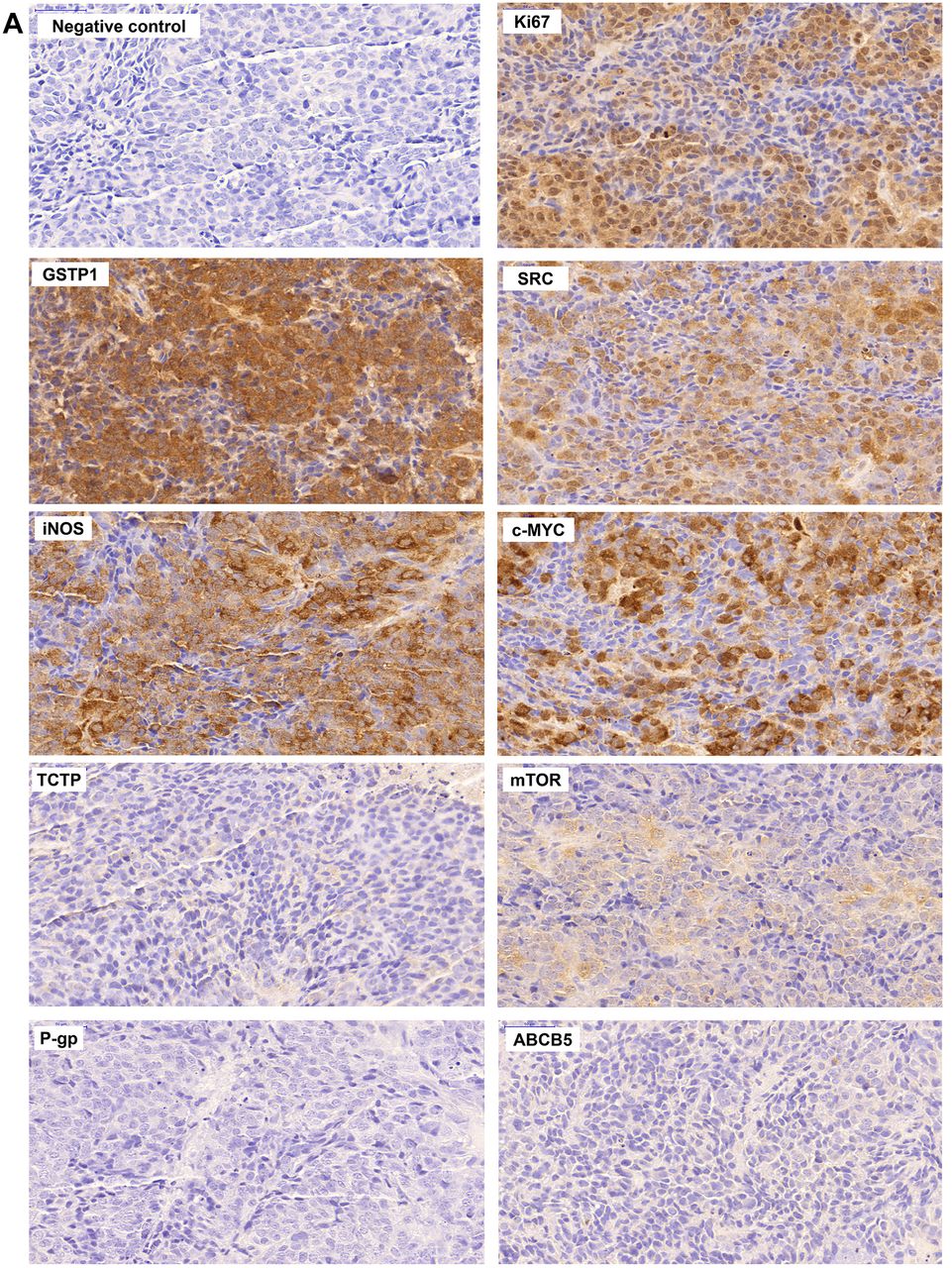
Immunohistochemistry staining. The immunostainings in the vaginal carcinoma were considerably different among the different biomarkers (Figure 2). Strong expression (>70% number of positive cells) was observed for glutathione S-transferase P1 (GSTP1), epidermal growth factor receptor (EGFR), inducible nitric oxide synthetase (iNOS), the transcription factor nuclear factor kappa B (NF-κB), the oncogene c-MYC, vascular endothelial growth factor (VEGF), and the proliferation marker Ki-67. Intermediate expression (around 50% number of positive cells) was found for the oncogene SRC, β-catenin, and the viral E7 protein while the expression of other markers investigated were either weakly (<10% number of positive cells) or not detected, i.e., the cell cycle-related translationally controlled tumor protein (TCTP), the transcription factor mammalian target of rapamycin (mTOR), the FLT-3, the transferrin receptor (CD71), the ATP-binding cassette (ABC) transporters ABCB5 and P-glycoprotein, the oncogene BRAF, the viral E6 protein, and the signal transducer PIK3R.

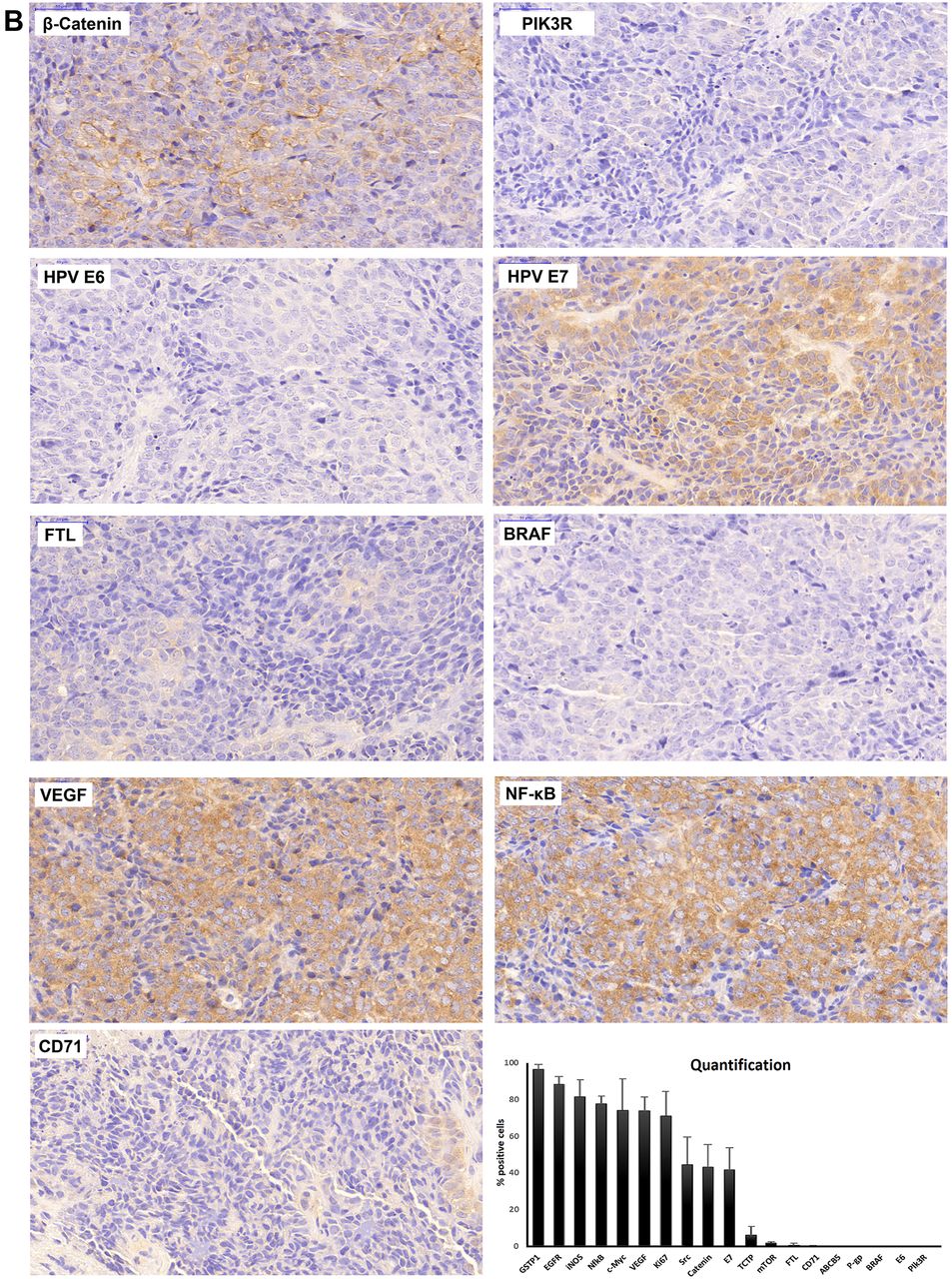
Immunohistochemical profiling of 19 biomarkers in a small cell carcinoma of the vagina. Magnification: ×20.
Virtual screening with FDA-approved drugs. As a next step, we downloaded the three-dimensional structures of the most expressed proteins in the vaginal tumor from the Protein Data Bank, i.e., GSTP1, EGFR, iNOS, NF-κB, c-MYC, VEGF, SRC, β-catenin, and HPV E7. The Ki-67 protein was not included in this analysis because it is usually applied in cancer pathology as a surrogate marker for proliferation but not used as a target for drug treatment. These protein structures were docked to 1,577 FDA-approved drugs in order to identify compounds that may bind and thereby inhibit these target proteins.
Table I shows a ranking list with the top 15 out of 1,577 compounds binding with the best affinity to the target proteins as determined by the PxRx program. In addition, we included well-known inhibitors of the corresponding proteins as positive control drugs. Inspecting all 9 target proteins, it can be seen that the top 15 compounds showed comparable or even better binding energies than the corresponding control inhibitors for these proteins indicating that the identified compounds might indeed exert inhibiting features to their targets.
PyRx-based virtual drug screening of FDA-approved drugs binding to target proteins strongly expressed in a case of small-cell vaginal carcinoma. The top 15 compounds out of 1,577 FDA-approved drugs with their free binding energies (kcal/mol) are shown.
To further refine the in silico results, we performed molecular docking with the AutoDock 4.2.6 program and determined the lowest binding energies (kcal/mol) and predicted inhibition constants (pKi, μM) of the top 15 compounds of each target protein (Figure 3). In addition to the binding energies, we also determined the predicted inhibition constants (pKi) and correlated both parameters with each other. We hypothesized that the free binding energies would correlate with the pKi values and used these correlations as quality control of our molecular docking analyses. We used the top 15 compounds for each of the 9 target proteins shown in Table II and subjected their binding energy and pKi values to the Pearson correlation test. Indeed, significant correlations between binding energies and pKi values were obtained for all 9 target proteins (Figure 3). However, three correlations deserved some caution. While the vast majority of all free energy/pKi value pairs assembled along linear regression lines, we found a few outliers for the linear regressions of GSTP1-, EGFR-, or VEGF-binding compounds, although each three independent molecular docking experiments have been performed for each target protein. The GSTP1 regression was statistically significant despite these outliers but not the regression analyses for EGFR or VEGF. If we removed these outliers from the EGFR and VEGF datasets (marked in black color in Figure 3), we obtained significant p-values with high correlation coefficients. This indicates that the molecular docking analyses generated reliable data in most but not all cases and that visual inspection is recommended to identify potentially useful drug candidates.

Molecular docking of each of the 15 candidate compounds on 9 different target proteins. The correlations between the lowest free energy (LBE, kcal/mol) and predicted inhibition constant values (pKi, μM) were calculated by the Pearson correlation test. The black-marked outliers in the EGFR and VEGF panels were not included in the correlation analyses.
FDA-approved drugs with cytotoxicity activity towards the NCI-60 panel of tumor cells. Their mechanisms of action, indications, side effects, and contraindications were compiled.
Then, we mined the database of the Developmental Therapeutics Program (DTP) of the National Cancer Institute (NCI, Bethesda, MD, USA) (21). This database contains the cytotoxicity data of more than 200,000 compounds tested in 60 cell lines of different tumor types. Such drugs were considered as possible candidates for treatment as they appeared among the top 15 best-binding compounds to each of the 9 proteins and also were cytotoxic against the NCI cell lines. We categorized the drugs as being weakly cytotoxic (log10IC50 between -4 and -5 M), intermediate cytotoxic (log10IC50 between -5 and -6 M), or strongly cytotoxic (log10IC50 <-6 M). Compounds with log10IC50 values >-4 M were excluded as being non-cytotoxic. As shown in Table II, some of these compounds are already approved cancer drugs, whereas others are drugs used to treat non-malignant diseases. The majority of drugs were bound with high binding affinity to more than one protein target, further supporting the drug repurposing concept that drugs already approved for specific diseases are not mono-specific and might, thus, qualify for the treatment of other diseases.
Discussion
In the present study, we describe a case of small cell vaginal carcinoma. Because this histology represents an extremely rare tumor type, large and reliable clinical trials about the optimal treatment options are not available. In such nonsatisfying situations, it is common sense to apply treatment protocols, which are used to treat small cell carcinoma of any location in the body. Therefore, it does not come as a surprise that without having better options at hand, current chemotherapy is hardly capable to cure patients with smallcell vaginal carcinoma.
The case presented here was also treated with usually applied anticancer drugs, including platin drugs (cisplatin, carboplatin), taxanes (paclitaxel), DNA topoisomerase I or II inhibitors (camptothecin, irinotecan, etoposide) in combination with or without radiotherapy. Chemotherapy and radiotherapy led to stabilization or slight regression of the disease at best. Therefore, new treatment options are urgently desired.
Precision medicine emerged as a new paradigm in tumor management during the past few years. As concepts for individualized therapy of small cell vaginal tumors are scarce, we performed immunohistochemical staining with 19 biomarkers (GSTP1, EGFR, iNOS, NF-κB, c-MYC, VEGF, Ki-67, SRC, β-catenin, HPV E6, HPV E7, TCTP, mTOR, FTL, CD71, ABCB5, P-gp, BRAF, and PIK3R) to identify single markers that are of relevance for the small-cell vaginal carcinoma of this specific patient. Seven proteins were strongly expressed (GSTP1, EGFR, iNOS, NF-κB, c-MYC, VEGF, Ki-67) and SRC, β-catenin and HPV E7 to a lesser extent. Based on these results, we asked the question, of whether drugs targeting these proteins could be identified. The other proteins were minimally or not expressed and were, therefore, not further considered for targeted therapy approaches.
The idea to exploit immunohistochemical protein expression profiling for targeted tumor therapy is different from a previous approach where we combined RNA-sequencing of a glioblastoma patient with a bioinformaticsbased virtual screening of FDA-approved drugs (22). The concept of drug repurposing is based on the observation that long-known drugs approved for one indication occasionally also show activity against other diseases (23-25).
The present study was designed to explore how novel treatment options could be developed for tumors without satisfying therapies. Since we identified compounds with known cytotoxic and anticancer activity on the one hand and clinical approval, on the other hand, it is realistic to consider such FDA-approved compounds for individualized compassionate use in the future. However, we also identified some drugs that are FDA-approved for other indications.
Interestingly, the anticancer drug imatinib was among the weakly cytotoxic compounds. This indicates that even weakly cytotoxic drugs could be considered for cancer treatment since most of the other drugs in the group of weakly cytotoxic compounds were not anticancer drugs but drugs used to treat other diseases. Examples include celecoxib, ergotamine, nystatin, saquinavir, and griseofulvin (26-29). Celecoxib is an anti-inflammatory drug. Since chronic inflammation is a contributing factor to cancer, it can be imagined that celecoxib might also exert anticancer effects (30). Ergotamine is an ergot alkaloid that is known for its activity against severe migraine. Due to its high toxicity, it does not qualify as an anticancer drug. Saquinavir is a virustatic drug, and saquinavir derivatives are further developed for cancer therapy (31). It is also known from other antimicrobial drugs that they exert anticancer activity. For instance, griseofulvin is an antimycotic that inhibits mitosis in both fungi and cancer cells (27, 28). Hence, antimicrobial drugs might bear some potential to be used for cancer therapy.
Among the FDA-approved drugs with intermediate cytotoxicity were ivermectin, loratadine, and pimozide. Ivermectin is preferentially used in veterinary medicine to treat parasites (nematodes, lice, mites). Although it specifically acts on glutamate-activated chloride channels of invertebrates, its anticancer activity has been documented in vitro and in vivo (32). Loratadine is a histamine receptor 1 (H1) antagonist that inhibited the growth of colon xenograft tumors by causing G2/M arrest of the cell cycle (33). Pimozide is an approved antipsychotic drug that inhibited stem-like cancer cells and has been proposed to be repurposed for cancer therapy (34, 35). The described cytotoxicity of these compounds might qualify them for their individualized use in patients who cannot be treated standard treatment because of refractory and therapy-resistant tumors. Despite the attractiveness of this approach, one should bear in mind that drugs approved for one disease and used off-label for a second disease might exert the main pharmacological effect towards the first disease as well as the unwanted side effects if used for the other disease. For illustration, if the ACE inhibitor telmisartan would be used for cancer therapy, its blood pressure-lowering activity might appear as a side effect in cancer patients.
The drugs appearing in the group of strongly cytotoxic compounds were all approved anticancer drugs (i.e., everolimus, irinotecan, ponatinib, sirolimus, teniposide), albeit for other tumor types than small-cell carcinoma of the vagina. Hence, their off-label use for the patient presented here seems to be obvious. Especially for refractory tumors to standard treatment, the use of approved anticancer drugs, which are established for other tumor types, represents a practical approach to possibly reach favorable treatment effects. In the case presented here, irinotecan was used to treat this vaginal carcinoma although this happened prior to and independently from our in silico analyses. Therefore, our bioinformatic drug repurposing approach may serve as a supportive measure for the individualized therapy of latestage cancer patients without further treatment options. In order to select which of these drugs might be appropriate for the treatment of the vaginal tumor presented here, it is not only important to consider the drug indications, possible anticancer activities, and mechanisms of action, but also their known side effects and contraindications. A compilation of these drugs regarding indication, mechanism of action, side effects, and contraindications is shown in Table II.
The patient presented here died in 2018, and our bioinformatics analysis was performed post mortem. Nevertheless, these results may serve as a first proof-of-principle to improve the treatment outcome of patients without any further treatment options from the standard treatment guidelines.
Small cell carcinoma of the vagina is an extremely rare tumor type, and only a few cases have been reported worldwide (36-41), and vaginal tumors are also very rare in Sudan (39). By contrast, cervix cancer as another gynecological tumor entity, is the second most common tumor type in females in Sudan (42) while it occurs much less frequently in Europe and the USA. Whether non-sufficient preventive measures (e.g., cervix cancer screening, vaccination) in Sudan compared to industrialized countries represent the only reasons for this discrepancy or whether specific cultural factors might also play a role, is worth to be considered. The etiology of vaginal tumors has been ascribed to exposure to diethylstilbestrol, infection with human papilloma or herpes simplex viruses, immunosuppressants, previous hysterectomy, cervical irradiation, or chronic irritations (3). While these risk factors are not known to apply to the patient presented here, another carcinogenic factor could be discussed.
The role of traditional incense burning (dukhan) in gynecological carcinogenesis is not clarified. Dukhan is widely distributed among married women in Sudan, especially among the older generations. Dukhan is a millennia-old tradition tracing back to ancient northeast African Kingdoms of Meroe and Nubia that were located in the present northern territories of Sudan. Dukhan is a ritual smoke bath generated by burning coals with perfumed acacia and sandalwood (Santalum paniculatum). The main purpose is to narrow the vagina, especially after childbirth. In combination with other plants such as Capparis decidua (tundub), it is also believed to help against joint and rheumatic pain, syphilis, and gonorrhea. Dukhan is also used as cosmetics for smoothening the skin. It is frequently combined with scented massage (termed dilka) to produce a pleasant scent of the skin, to let the skin look tanned yellowish and shiny, and to exert anti-microbial effects. For dilka, scented oils (karkar) and ointments (kabarait) are prepared from different ingredients (sandalwood, talh, shaff, mahlab, qurunful, kilait, musk, sugar, and liquid perfumes).
It is apparent that hot smoke can cause skin irritations. A recent study reported on 11 women taking dukhan smoke baths containing wood from Acacia seyal and Terminalia brownii suffered from brown-erythematous excoriated papules, plaques, and lichenification at the sites exposed to dukhan. These symptoms were diagnosed as contact dermatitis (43). Since chronic inflammatory conditions are well-known factors contributing to carcinogenesis, it can be speculated that the carcinogenic substances of the burned woods in dukhan might at least in part contribute to the development of vaginal tumors such as the case presented here. Although a direct causal link between dukhan and vaginal carcinogenesis is still missing, such a speculation can at least be considered. The role of traditional practices such as dukhan for gynecological carcinogenesis deserves further investigation in the future.
In conclusion, we described a rare case of a small-cell vaginal carcinoma. This tumor entity is of limited responsiveness to standard chemo- and radiotherapy and successful treatment options are rare. In this situation, we searched for an approach to identify theoretical alternatives for treatment. For this reason, we performed immunohistochemistry on a large panel of biomarkers using a biopsy of this tumor. The biomarkers whose protein expression was most upregulated were considered as potential drug targets.
Using virtual screening with PyRx and molecular docking with AutoDock 4.2.6, we screened a library of 1,577 approved drugs in an attempt to identify known drugs originally approved for other medical purposes. Following this immunohistochemistry- and bioinformatics-guided drug repurposing approach, we found several FDA-approved drugs that are not routinely considered for small-cell vaginal carcinoma treatment. These drugs might be effective even in situations where the available standard therapies fail. This drug repurposing approach might be theoretically not only applicable to small-cell vaginal carcinoma but to other refractory tumor entities as well. This concept represents a novel possibility for individualized tumor therapy that deserves further exploration in the future.
Footnotes
Authors’ Contributions
M.E.M.S. performed the experiments; H.E.K. contributed to the design of the paper; S.K.T. was involved in the clinical management of the patient; T.E. designed and wrote the paper.
Conflicts of Interest
T.E. is co-inventor of patent #EP18211231. The other Authors do not have any potential conflict of interest in relation to this study.
- Received March 15, 2022.
- Revision received April 4, 2022.
- Accepted April 5, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.