


Abstract
Background/Aim: Heterogeneous nuclear ribonucleoproteins (hnRNPs) contribute to multiple cellular functions including RNA splicing, stabilization, transcriptional and translational regulation, and signal transduction. However, the prognostic importance of genetic variants of hnRNP genes in clinical outcomes of prostate cancer remains to be elucidated. Patients and Methods: We studied the association of 78 germline single-nucleotide polymorphisms (SNPs) in 23 hnRNP genes with the overall survival (OS), cancer-specific survival (CSS), and progression-free survival (PFS) in 630 patients with prostate cancer receiving androgen-deprivation therapy (ADT). Results: PTBP1 rs10420407 was the most significant SNP (false discovery rate q=0.003) and carriers of the A allele exhibited poor OS, CSS, and PFS. Multivariate Cox analysis confirmed PTBP1 rs10420407 A allele was an independent negative prognostic factor for OS and PFS. Expression quantitative trait loci analysis showed that the rs10420407 A allele had a trend towards increased PTBP1 mRNA expression, and higher expression was correlated with prostate cancer aggressiveness and poor patient prognosis. Meta-analysis of 16 independent studies further indicated a tumorigenic effect of PTBP1, with a higher expression in prostate cancers than in adjacent normal tissues (p<0.001). Conclusion: Our data suggest that PTBP1 rs10420407 may influence patient response to ADT, and PTBP1 may be involved in the pathogenesis of prostate cancer progression.
- Androgen-deprivation therapy
- heterogeneous nuclear ribonucleoprotein
- meta-analysis
- prostate cancer
- PTBP1
- survival
Prostate cancer is the second-most common cancer affecting men worldwide, with 1.4 million new cases in 2020 (1). Since androgen signalling affects the proliferation and differentiation of the normal prostate epithelium, and stimulates prostate cancer cell growth, androgen-deprivation therapy (ADT) is used as a common and effective treatment for patients with advanced prostate cancer (2). However, the disease inevitably progresses to castration-resistant prostate cancer (CRPC) despite continuous hormonal regulation; patients with metastatic CRPC have a poor prognosis with a median survival time of 16-18 months (3). Genetic and environmental factors are believed to contribute to the development of prostate cancer; a risk of developing the disease increases with age, having an African ancestry, North American or northern European location, and positive family history (4). A recent study estimated that 57% of the variability in prostate cancer risk is attributed to genetic factors, and it is recognised as one of the most heritable cancers (5). The variations in critical genes of individuals may explain the variable patient outcomes, and the use of this information may help determine the treatment response, and guide optimal dose or patient selection.
Heterogeneous nuclear ribonucleoproteins (hnRNPs) are a family of proteins comprising more than 20 major RNA-binding proteins that are responsible for post-transcriptional control of RNA, such as pre-mRNA splicing and polyadenylation, and functional mRNA export, turnover, and translation (6). The amino terminus of hnRNPs contains an RNA recognition motif that binds to pre-mRNA sequences, and the carboxyl terminus contains a glycine-rich domain that interacts with other hnRNPs (7). The hnRNPs generally bind to exonic and intronic splicing silencers to inhibit or promote splicing reactions by regulating the assembly of the spliceosome complex or the recruitment of serine/arginine-rich proteins to the splicing sites (8). Recent studies demonstrated that the expression of hnRNPs is commonly deregulated in multiple cancer types including prostate cancer. HNRNPA1, HNRNPA2, and polypyrimidine tract binding protein 1 (PTBP1) have been demonstrated to be up-regulated by the MYC proto-oncogene, which induces the production of pyruvate kinase to activate aerobic glycolysis in cancer cells (9). A high expression of several hnRNPs is observed in prostate cancers compared to that in benign prostate tissues (10, 11). Studies have shown that HNRNPK plays a role in the regulation of androgen receptor (AR) expression via transcriptional and post-transcriptional mechanisms (12, 13). Additionally, HNRNPK is found to be co-localized with AR in a complex inside the nucleoplasm, and both proteins are modulated via treatment with the anti-androgen bicalutamide (14). Moreover, a family-based study found that a variant in the regulatory region of HNRNPA0 is associated with elevated cancer incidence (15).
The genetic variants of hnRNP genes are thought to influence gene expression; however, it is still unknown whether hnRNP single nucleotide polymorphisms (SNPs) play a role in prostate cancer prognosis. In the present study, we systematically selected haplotype-tagging SNPs (htSNPs) to capture gene-wide common variations, and evaluated their associations with survival outcomes in patients with prostate cancer after receiving ADT.
Patients and Methods
Patient and response evaluation. The study population comprised 630 Taiwanese patients with advanced prostate cancer receiving ADT in three medical centres in Taiwan: Kaohsiung Medical University Hospital, Kaohsiung Veterans General Hospital, and National Taiwan University Hospital. The patient inclusion and exclusion criteria have been described previously (16, 17). Detailed clinicopathological information was obtained from the patient medical records. The cause and date of death were obtained by linking the personal identification number with the National Death Registry via the Ministry of Health and Welfare, Taiwan. Overall survival (OS) was defined as the time from the initiation of ADT to death from any disease. Cancer-specific survival (CSS) was defined as the duration from the initiation of ADT until death due to cancer. Progression-free survival (PFS) was defined as the time from ADT initiation to tumour progression or cancer-related death. This study was approved by the institutional review board of Kaohsiung Medical University Hospital (KMU HIRB-2013132), and was conducted in accordance with the Good Clinical Practice guidelines. All patients provided written informed consent prior to the study enrolment.
SNP selection and genotyping. The htSNPs within 23 hnRNP genes and their 5-kb flanking regions were obtained from the 1000 Genomes data for Han Chinese in Beijing, China, and Southern Han Chinese with a threshold of minor allele frequency (MAF) of at least 0.03 and an r2 threshold of 0.8 (18). Genomic DNA was extracted from the peripheral blood, and the Affymetrix Axiom Genotyping Arrays system (Thermo Fisher Scientific, Waltham, MA, USA) was used for genotyping at the National Centre for Genome Medicine, Taiwan, as described previously (19). Any htSNPs that showed a genotyping call rate of <0.9, MAF of <0.02, and a Hardy-Weinberg equilibrium of <0.001 was excluded, leaving 78 htSNPs for further analyses.
Bioinformatics analysis. We performed functional annotation of the identified htSNPs using HaploReg v4.1 (20). The expression quantitation trait loci analysis between identified htSNPs and PTBP1 gene expression levels was evaluated using HapMap3 lymphoblastoid cell data (21). Differential expression of PTBP1 mRNA in prostate cancer tissues and adjacent normal tissues was analysed using the Oncomine database (22) and The Cancer Genome Atlas Prostate Adenocarcinoma (TCGA PRAD) data (23).
Statistical analysis. Statistical analyses were performed using the SPSS software version 19.0.0 (IBM, Armonk, NY, USA). A two-sided p<0.05 was considered significant, and multiple testing correction procedures and q values (24) were also applied to report the false discovery rate with a threshold of 0.05. Meta-analysis of gene expression studies on prostate cancer was expressed as standardized mean difference (SMD), and combined with a model of random effects using RevMan 5.4.1 (Cochrane, London, UK).
Results
Study participant characteristics. The clinical characteristics of the study population are summarized in Table I. In total, 414 (65.7%) patients died, 314 (49.8%) patients died from cancer, and 518 (82.6%) showed disease progression with a median follow-up time of 165.8 months. The age, stage, Gleason score at diagnosis, prostate-specific antigen (PSA) level at ADT initiation, PSA nadir, and time to PSA nadir displayed significant associations with OS, CSS, and PFS in patients with advanced prostate cancer treated with ADT.
Clinicopathologic characteristics of the study population.
Association between hnRNP SNPs and the clinical response to ADT in patients with prostate cancer. The associations between each candidate htSNP and the three clinical outcomes are presented in Table II. Two PTBP1 htSNPs called rs10420407 and rs11549883 that were in strong linkage disequilibrium (r2=0.98), showed significant associations (q<0.05) with OS following ADT. PTBP1 rs10420407 was the most significant SNP, and patients carrying the A allele had a worse OS than those with a GG genotype [hazard ratio (HR)=1.96, 95% confidence interval (CI)=1.42-2.71, p=0.000038, Table III and Figure 1A). Multivariate analysis results were consistent with this association after adjusting for age, stage, Gleason score at diagnosis, PSA at ADT initiation, PSA nadir, and time to PSA nadir (HR=1.64, 95% CI=1.18-2.30, p=0.004, Table III). Notably, patients carrying the A allele of PTBP1 rs10420407 also had a worse CSS (via univariate analysis) and PFS (via both univariate and multivariate analyses) than those with a GG genotype (Table III and Figure 1B and C).
HnRNP SNPs and the p-values of their associations with OS, CSS, and PFS in patients with prostate cancer treated with ADT.
The association of PTBP1 rs10420407 with OS, CSS, and PFS in prostate cancer patients receiving ADT.
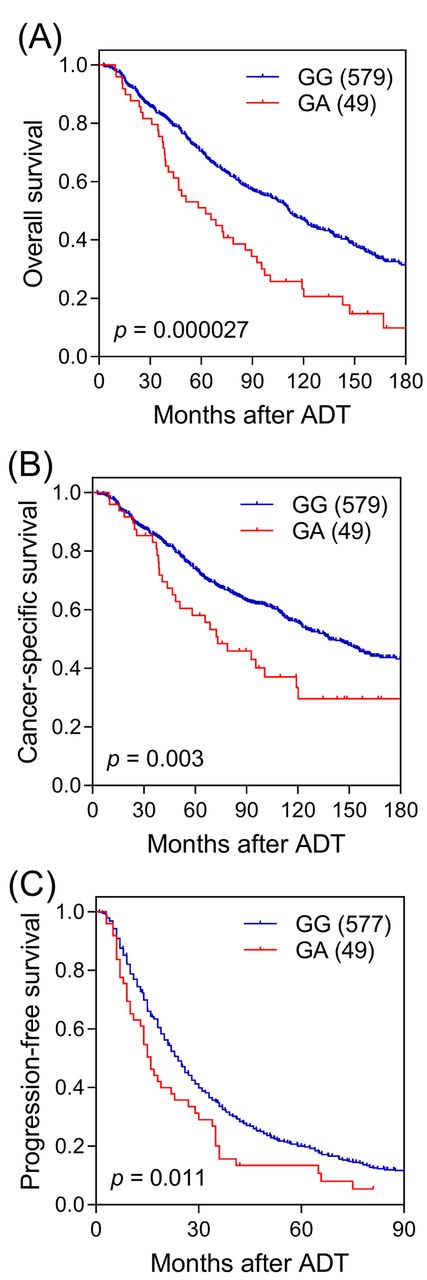
Kaplan-Meier curves for (A) overall survival, (B) cancer-specific survival, and (C) progression-free survival depending on PTBP1 rs10420407 genotypes. Values in brackets represent the number of patients. ADT: androgen-deprivation therapy.
Functional analyses of PTBP1 variants in prostate cancer. To investigate the functional importance of PTBP1 rs10420407 in prostate cancer progression, we first performed functional annotation using HaploReg. The analysis showed that rs10420407 and rs11549883 were situated in regulatory regions associated with active enhancers, DNase hypersensitivity, and RNA polymerase II binding, which indicated a high likelihood of affecting PTBP1 gene expression (Table IV). Using HapMap3 lymphoblastoid cell data, a suggested association with PTBP1 expression was observed in rs10420407, with the risk variant allele A, associated with higher PTBP1 expression (p=0.076, Figure 2A). By analysing a TCGA PRAD dataset, we further evaluated the prognostic value of PTBP1 in patients with prostate cancer. A higher PTBP1 expression was found in patients with prostate cancers, and the expression was progressively higher as the Gleason score and stage of cancer increased (p<0.001, Figure 2B, C and D). Furthermore, the higher expression of PTBP1 not only showed a trend of correlation with poor PFS (Figure 2E), but was significantly correlated with a poor disease-free survival in patients with prostate cancer (p=0.034, Figure 2F). The clinical relevance of PTBP1 was confirmed via meta-analysis of 16 gene expression datasets, comprising a total of 1,152 prostate cancer cases and 326 adjacent normal tissues. PTBP1 in prostate cancers was significantly and consistently up-regulated than in normal tissues (SMD 0.73, 95% CI=0.45-1.02, p<0.001, Figure 2G). These data suggested that PTBP1 may be functionally important in the pathogenesis of prostate cancer.
Functional annotation of PTBP1 rs10420407 and rs11549883.

Functional analyses of PTBP1 in prostate cancer. (A) rs10420407 A allele correlates with an increasing PTBP1 expression based on HapMap3 lymphoblastoid cell data. PTBP1 was overexpressed in (B) cancer, (C) high Gleason score, and (D) more advanced stage tumours in TCGA PRAD data. Patients with a high PTBP1 expression tend to have a worse (E) progression-free survival and (F) disease-free survival compared to those with a lower PTBP1 expression. (G) Meta-analysis of 16 studies showed that the expression level of PTBP1 was significantly higher in prostate cancer than in normal tissues. Values in brackets represent the number of patients. TCGA PRAD: The Cancer Genome Atlas Prostate Adenocarcinoma. Rho: Spearman’s rank correlation coefficient. SD: standard deviation. IV: inverse variance. CI: confidence interval.
Discussion
In the present study, we applied multiple strategies, including a haplotype tagging approach to improve SNP coverage, false discovery rate to adjust for multiple comparisons, and meta-analysis and functional annotation to systematically evaluate the clinical significance of hnRNPs in prostate cancer. We found that two htSNPs in PTBP1 were associated with poor clinical outcomes in patients with prostate cancer receiving ADT. Furthermore, functional analysis of independent gene expression studies indicated that an increased expression of PTBP1 was correlated with advanced pathological features and worse survival after treatment for prostate cancer. To the best of our knowledge, this is the first report showing the clinical relevance of PTBP1 in the progression of prostate cancer.
According to our genetic association analysis, the strongest signals corresponded to two highly correlated SNPs (r2=0.98): rs10420407, which is an intronic SNP, and rs11549883, which is a synonymous SNP in an exon of PTBP1. Functional annotation indicated that rs10420407 and rs11549883 were located in a region with histone modifications associated with active transcription of PTBP1, suggesting that these risk loci may influence PTBP1 expression and alter its biological fate. However, additional fine-mapping and functional studies are needed to identify the true causal variants and how they disrupt molecular mechanisms contributing to prostate cancer progression.
PTBP1, belonging to the PTB family of hnRNPs, functions as a regulator of post-transcriptional gene expression by preferentially binding to polypyrimidine-rich stretches of RNA, and is expressed in almost all cell types (25). PTBP1 has been demonstrated to promote cancer progression and regulate apoptosis via several important cancer-associated pathways, such as the epidermal growth factor (26), mitogen-activated protein kinase (27), and phosphoinositide 3-kinase/protein kinase B pathways (28). PTBP1 also regulates hypoxia inducible factor-1α signalling to alter renal cancer cell migration, invasion, and angiogenesis (29). Moreover, PTBP1 alters pyruvate kinase splicing, leading to an increase in the pyruvate kinase M2 (PKM2)/PKM1 isoform ratio that favours uncoupled glycolysis, a cancer-specific energy metabolism state (9). This PTBP1/PKM2 pathway is found to promote glycolysis, increase cell proliferation, and induce resistance to cell death in multiple tumour types (30). Along with these results, we demonstrated that PTBP1 is up-regulated in prostate cancer and is associated with poor patient prognosis. However, the exact mechanisms of the role of PTBP1 in prostate cancer progression remain to be elucidated.
While this study presents the first comprehensive analysis on the role of genetic variants of hnRNP genes in prostate cancer and the efficacy of ADT, it has certain limitations. First, this was a retrospective study; therefore, the results need to be replicated in prospective clinical trials. Second, the sample size was moderate, and more validation cohorts are required to confirm our findings. Third, we only analysed the common genetic variants (MAF>0.03), which might have led to the omission of important low frequency variants. Additionally, all the participants in this study are Taiwanese individuals and these findings may not apply to patients of different ethnicities. Finally, the functional analyses were based on the publically available datasets; additional experiments are needed to elucidate the molecular mechanisms of PTBP1 in prostate cancer.
In conclusion, our study provides evidence that PTBP1 rs10420407 is significantly associated with the efficacy of ADT, and patients with a high expression of PTBP1 demonstrate poor survival. Specific genetic variations in conjunction with gene expression and tumour features may help in the selection of patients with prostate cancer who may benefit from ADT or other therapies.
Acknowledgements
This work was supported by the Ministry of Science and Technology of Taiwan (grant nos: 108-2314-B-037-029, 108-2314-B-037-026-MY2, 108-2320-B-039-050-MY3, 109-2314-B-037-108-MY2, and 109-2314-B-037-106-MY3), the Kaohsiung Medical University Hospital (grant nos: KMUH105-5R42, KMUH108-8R53 and KMUH108-8R55), the Kaohsiung Medical University Research Center (grant no: KMU-TC108A04-4), and the China Medical University (grant nos: CMU108-MF-50, CMU109-SR-64, and CMU109-MF-65). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. We thank Chao-Shih Chen for data analysis, and the National Center for Genome Medicine, Ministry of Science and Technology of Taiwan, for technical support. The results published here are based in part on data generated by the HaploReg, HapMap, 1000 Genomes, and TCGA projects.
Footnotes
* These Authors contributed equally to this work.
↵Authors’ Contributions
S-PH, C-YH, C-CY, VCL, and B-YB conceptualized and designed the study. S-PH, L-CC, and B-YB performed the experiments. L-CC, Y-TC, C-HL and T-LL coordinated and supervised data collection. S-PH, L-CC, Y-TC, and B-YB performed the analysis. All the Authors drafted, reviewed and approved the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no conflicts of interest in regard to this study.
- Received February 12, 2021.
- Revision received March 2, 2021.
- Accepted March 3, 2021.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}