


Abstract
Background/Aim: Cetuximab in combination with chemotherapy is recommended as first-line therapy for metastatic colorectal cancer (mCRC) with wild-type RAS. However, drug resistance to cetuximab exists widely in mCRC and reduces the prognosis of patients. Although some genomic alterations have been demonstrated to drive acquired resistance to cetuximab, the overall compendium of inherent molecular mechanisms is still incomplete. Materials and Methods: Four liver metastasis biopsies were collected from two mCRC patients who were treated with cetuximab in combination with 5-fluororacil plus leucovorin and oxaliplatin (FOLFOX) regimen. Results: Transcriptomic analysis revealed global gene expression alterations between paired samples prior to treatment and after acquired resistance. Further bioinformatics analysis discovered differentially expressed protein-coding genes/lncRNAs/miRNAs, potential miRNA-mRNA regulatory networks and lncRNA-mRNA competing endogenous RNA network, which may be potential biomarkers or play roles during the process of acquired resistance to cetuximab. Conclusion: Our study contributes to deciphering the molecular mechanisms of acquired resistance to cetuximab.
Colorectal carcinoma (CRC) is one of the most common cancers and has the third leading incidence rate worldwide. About 1.2 million people are newly diagnosed with colorectal cancer per year (1). Distant metastasis is the main reason for death in CRC patients. About 25% of CRC patients have distant metastasis at first diagnosis, and 50% of stage I to stage III patients will eventually develop metastasis (2). Liver is the main target organ of metastasis in colorectal cancer (mCRC), and the majority of CRC patients with liver metastases are unable to get radical resection. For these patients, the main purpose of treatment is to prolong survival, prevent further tumor progression, reduce tumor-related symptoms and improve quality of life (2).
In recent years, the application of chemotherapy and molecular targeted therapies, including anti-epidermal growth factor receptor (EGFR) monoclonal antibodies and anti-vascular endothelial growth factor (VEGF) monoclonal antibodies, has improved the prognosis of mCRC patients. The National Cancer Institute lists 24 drugs for the treatment of mCRC (see list in http://www.cancer.gov/about-cancer/treatment/drugs/colorectal), among which cetuximab is one of the most effective monoclonal antibodies targeting EGFR on the cell membrane (3) and can significantly improve the prognosis of mCRC patients with wild-type RAS (4-9). Cetuximab in combination with chemotherapy has been recommended as first-line therapy (10).
However, drug resistance to cetuximab exists widely. Clinical studies show that cetuximab alone is effective for only about 10% of mCRC patients (7). Many efforts have been made to find biomarkers or drivers of drug resistance to cetuximab, in order to increase the effectiveness of cetuximab and improve the treatment of mCRC. Drug resistance to cetuximab can be classified into primary and secondary resistance (i.e. acquired resistance). The main causes of primary drug resistance are mutations in codons 12 and 13 at the exon 2 of the KRAS gene (6, 11-13), which has been used for routine testing and guiding the clinical treatment (8, 10). Moreover, several other genomic alteration events, including mutations in KRAS exons 3 and 4, NRAS exon 2, 3 and 4, BRAF V600E, PIK3CA and HER2 amplification, have also been reported to be associated with primary drug resistance to cetuximab (14-18). Acquired resistance to cetuximab often occurs at 3 to 12 months after effective response to treatment (7). Mutations in KRAS and NRAS genes are the most common causes for acquired resistance to cetuximab (19, 20). The amplification of HER2 and MET genes, the other two members of the receptor tyrosine kinases (RTK), can also lead to acquired resistance by activating downstream RAF-MEK-ERK signaling pathway (21, 22). In addition, the S492R mutation in the extracellular domain of EGFR can also result in acquired resistance by hindering antibodies from binding to EGFR (23).
Although some genomic alterations have been identified and demonstrated to drive acquired resistance to cetuximab, the overall compendium of inherent molecular mechanisms is still incomplete. Transcriptomic analysis can provide comprehensive insights into molecular mechanisms, which include differential expression analysis and pathway/regulation networks of protein-coding genes, long non-coding RNAs (lncRNA) and miRNAs. However, transcriptome alterations, especially alterations between matched biopsies prior to treatment and after acquired resistance, are largely unknown up to date.
In this study, we collected four liver metastasis biopsies from two mCRC patients who were treated with cetuximab in combination with 5-fluororacil plus leucovorin and oxaliplatin (FOLFOX). Each patient had undergone ultrasound-guided biopsies prior to treatment and after acquired resistance (tumor re-progression after effective response to treatment for more than six months). High-throughput transcriptome sequencing, including RNA-Seq and small RNA-Seq, were conducted for all the four samples. Transcriptomic analysis revealed gene expression alterations between paired samples prior to treatment and after acquired resistance. Further bioinformatics analysis discovered differentially expressed protein-coding genes/lncRNAs/miRNAs, potential miRNA-mRNA regulatory networks and lncRNA-mRNA competing endogenous RNA (ceRNA) network, which may be potential biomarkers or play roles during the process of acquired resistance to cetuximab. Our study may contribute to deciphering the molecular mechanisms of acquired resistance to cetuximab.
Materials and Methods
Patient inclusion and sample collection. A retrospective single-center study was performed at the 307 Hospital, Academy of Military Medical Sciences, Beijing, China. Eligible patients had pathologically confirmed metastatic colorectal cancer (mCRC) harboring wild-type KRAS codons 12 and 13 and BRAF codon 600 determined via Sanger sequencing of the tumor tissue DNA, and they received targeted therapy and chemotherapy for the first time. Patients received cetuximab in combination with FOLOX chemotherapy. Computed tomography (CT) scans were performed and reviewed every 4 to 6 weeks to evaluate clinical response using the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1 (24). All the patients signed an informed consent for liver biopsy and publication of the results. Fresh tumor tissues from metastatic liver lesions were obtained at baseline and disease progression. Tumor biopsies were frozen at liquid nitrogen immediately when taken out and were linked to demographic, clinical and genetic data stored in a secure research database. This study protocol was approved by the local ethics committee (KY-2011-8-3). Tissue acquisition and handling of human tissue specimens were carried out in accordance with the institutional and state regulations.
Treatment of cetuximab in combination with chemotherapy. All of these agents were administered intravenous (IV) via an ambulatory pump and a central venous line. Treatment was continued until disease progression. Cetuximab: 400 mg/m2 IV over 2 h at the first week as an initial dose, then 250 mg/m2 IV over 1 h weekly. FOLFOX regimen: Oxaliplatin 85 mg/m2, IV over 2 h, day 1; Leucovorin 400 mg/m2, IV over 2 h, day 1; 5-fluorouracil 400 mg/m2, bolus on day 1, then 2,400 mg/m2 IV infusion over 46 h.
Liver biopsy and pathology assessment. Ultrasound guided liver biopsies were performed using a 18 gauge biopsy needle, 2 cores with a minimum length greater than 5 mm were taken, and each of the cores were mirror sectioned, half of which were send to pathology department for H&E staining and pathological evaluation to ensure the tumor content was more than 50%. The rest of the tissue was placed in a freezing tube with RNAlater, frozen at −80°C.
RNA isolation, library construction and RNA sequencing. Total RNA was isolated from fresh frozen tumor tissues using Trizol reagent. Library constructions of Poly-A mRNA and small RNA were conducted using TruSeq Stranded mRNA Library Prep Kit (Illumina, San Diego, CA, USA) and TruSeq Small RNA Library Preparation Kits (Illumina, USA). The high-throughput sequencing was carried out using Illumina Hiseq 2000.
Mapping and quantification. For mRNA sequencing data, poor quality reads were filtered from the raw paired-end reads using custom perl script. Then the paired-end reads were aligned to the hg19 human genome assembly using Tophat program version 2.0.13 (25). The resulting alignments were saved as a BAM file. The raw counts for each gene were calculated using the HTSeq-count script (26) by counting the number of reads overlapping with genes (mRNAs and lncRNAs) annotated in GENCODE version 15 (27). For small RNA sequencing data, after removing adaptors and poor quality reads, small RNA reads were aligned to know human miRNAs from miRBase v21 (28). The raw count for each miRNA was calculated. The workflow is illustrated in Supplementary Figure 1.

Pathological sections and CT scans of liver lesions. (A) H&E staining picture of primary tumor of colon (left) and liver metastasis (right). (B) Tumor response to cetuximab containing therapy in patient mCRC002 with liver metastases. CT scan revealed multiple heterogeneously enhancing tumor masses in the right and left lobes of liver, after 2 cycles (8 weeks) of chemotherapy plus Cetuximab, dramatic tumor regression at all sites of disease were seen, the regression lasted 24 weeks. After continued therapy for more than 7 months, the patient developed disease progression.
Estimation of tumor purity. Tumor purity of the four samples was estimated using the ESTIMATE R package (29). ESTIMATE method uses gene expression profiles of 141 immune genes and 141 stromal genes to obtain ESTIMATE scores and purity was estimated using the formula described in Yoshihara et al. (29).
Categories and subcellular localization of protein-coding genes. Significantly up-regulated genes after acquired resistance were assigned to different categories and subcellular localizations according to Uniprot database (30).
Literature search. The combination of gene name and any of these keywords, including “cancer”, “tumor”, “resistant”, “resistance”, “anti-drug” and “drug-resistance”, were used in PubMed literature search. According to the results of the literature search, differentially expressed genes were manually classified into five groups, which are tumor-related genes (“cancer” and “tumor”), drug resistance-related genes (“resistant”, “resistance”, “anti-drug” and “drug-resistance”), drug resistance genes (“resistant”, “resistance”, “anti-drug” and “drug-resistance”), tumor suppressor genes (“cancer” and “tumor”) and other genes.
Construction of miRNA-mRNA negative regulatory network and ceRNA network. miRwalk (31), at default settings, was used to predict target mRNAs for each differentially expressed miRNA. The potential target mRNAs, which were supported by at least three prediction methods of miRwalk, RNA22, miRANDA and Targetscan and differentially expressed in opposite direction of the miRNA, were retained. Then, these potential regulatory links between miRNAs and mRNAs with significant opposite expression were used for construction of a miRNA-mRNA negative regulatory network.
Based on gene annotations of GENCODE v15 (27), we selected lncRNAs with the given “gene_type”, including lincRNA, antisense RNA, sense intronic, overlap sense and processed_transcript. The ceRNA prediction procedure includes four steps (Supplementary Figure 2): i) predicting the lncRNA-miRNA interactions based on the CLIP-Seq data from Starbase database (Version 2.0) for differentially expressed lncRNA; ii) obtaining experiment validated miRNA-mRNA pairs based on the miRtarbase database for differentially expressed mRNAs; iii) generating potential lncRNA-mRNA relationships connected by miRNAs; iv) excluding lncRNA-mRNA pairs which showed expression changes in different directions. Cytoscape was employed for visualization of networks.
Availability of data and material. Raw data and gene expression profiles for this study are accessible via the GEO repository (http://www.ncbi.nlm.nih.gov/geo/) under accession identification number GSE84270. Supplementary tables and supplementary figures can be downloaded from http://www.omicsnet.org/pub/coloncancer.html.
Statistical analysis. For gene or miRNA differential expression analysis, paired sample design was employed using R package DESeq2 version 1.8.0 (32), which was a powerful method for the detection of differentially expressed genes of count data from RNA-Seq using shrinkage estimation for dispersions and fold changes to improve stability and interpretability of estimates. Fold change >1.5 and FDR <0.05 was adopted as a statistically significant threshold. The variance Stabilizing Transformation function was used to normalize the count data for visualization.
Results
Clinical and treatment information of patients. Two patients who were newly diagnosed and pathologically confirmed with metastatic colorectal cancer (mCRC) harboring wild-type KRAS codons 12 and 13 and BRAF codon 600 were screened for eligibility between August 2011 and December 2013. They were treated with cetuximab in combination with FOLFOX regimen (see Materials and Methods) and obtained continuous partial responses for more than six months. CT scans of liver lesions were performed every four to six weeks. The scans at baseline, best response and disease progression are shown in Figure 1. Detailed clinical and treatment information were provided in Supplementary Table I.
Transcriptome expression profiles of four mCRC biopsies. The four biopsy samples were evaluated by two pathologists and tumor purities were confirmed to be greater than 50%. Each biopsy sample was subjected to high-throughput RNA and small RNA sequencing to obtain expression profiles of genes (protein-coding genes and lncRNAs) and miRNAs. We evaluated the tumor purity scores using ESTIMATE algorithm (29) and gene expression profiles. The tumor purity scores of the four samples ranged from 0.79 to 0.92 (Supplementary Table II), ensuring the reliability of the analysis results. Next, we compared gene and miRNA expression levels between paired samples of prior treatment and after acquired resistance for each patient (Figure 2). The results showed that many genes (Figure 2A and B) and a few miRNAs (Figure 2C and D) were significantly up- or down-regulated in the two patients after drug resistance occurred.
Differentially expressed protein-coding genes after acquired resistance to cetuximab. We identified 782 protein-coding genes differentially expressed between biopsy samples of prior treatment and after acquired resistance. Among them, 699 genes were up-regulated in the biopsy samples after acquired resistance and 83 genes were down-regulated (Figure 3A, Supplementary Table III). The up-regulated gene number is eight times greater than that of the down-regulated genes. Moreover, the change folds of up-regulated genes are much greater than those of the down-regulated genes (11.17±0.64 vs. 5.23±0.29, p<0.001, Mann-Whitney U-test). Specifically, 282 genes were up-regulated by >10 fold and an adjusted p-value <0.01, covering 40.3% (282/699) of all the up-regulated genes, whereas only 5 genes were down-regulated by >10 fold and adjusted p value <0.01, covering 6.0% of all the down-regulated genes. These data show that many more genes were activated than repressed when resistance occurred.
GO annotation and KEGG pathway enrichment analysis was then performed on 699 significantly up-regulated genes and 83 down-regulated genes using DAVID webserver (33, 34), respectively. The top five up-regulated biological processes were: small molecule metabolic process, oxidation-reduction process, xenobiotic metabolic process, regulation of complement activation, and negative regulation of endopeptidase activity. The top five enriched up-regulated KEGG pathways were: complement and coagulation cascades, metabolic pathways, chemical carcinogenesis, glycine, serine and threonine metabolism, and retinol metabolism (Figure 3B). These results showed that metabolism and complement activity are more active after resistance to cetuximab occurred, which is consistent with the previous reports showing that metabolic alterations help cancer cells to proliferate rapidly and develop drug resistance phenotypes (35, 36). However, the down-regulated genes had no enriched biological processes or KEGG pathways.
Four keratins, KRT1, KRT14, KRT5 and KRT2, were most significantly up-regulated among all the up-regulated genes (Supplementary Table III). The change folds were all greater than 110, far greater than those of other up-regulated genes. KRT1, KRT2 and KRT5 are type II cytokeratins and KRT14 is a type I cytokeratin. KRT5 and KRT14 are usually expressed in the basal layer of the epidermis and stratified squamous epithelia, and form heterotetramers. KRT5 and KRT14 are diagnostic markers in breast cancer (37), and their high expression indicates aggressive behavior and poor prognosis (38, 39). KRT1 is a diagnostic marker in skin squamous cancer (37). Our result suggests that KRT1, KRT2, KRT5 and KRT14 may be markers of resistance to cetuximab in mCRC.

Comparisons of gene and miRNA expression between paired samples of prior treatment and after acquired resistance for each patient. Scatterplots of gene and miRNA expression between paired samples prior to treatment and after acquired resistance for mCRC001 (A for genes and B for miRNAs) and mCRC002 (C for genes and D for miRNAs). Grey line stands for y=x; red line stands for y=x+2; green line stands for y=x−2. In panel A for example, black points above red line account for genes up-regulated more than twice in the acquired resistance sample, while black points under green line account for genes down-regulated more than twice in the acquired resistance sample. Histograms alongside each scatterplot show distributions of gene and miRNA expression of corresponding samples (cyan is for sample of prior treatment and brown for acquired resistance).
We further inspected the kinases, cytokines and cell surface receptors in the up-regulated genes (Figure 3C), since they can more readily become drug targets. Two nuclear receptors, ESR1 (Estrogen receptor 1) and AR (Androgen receptor), were up-regulated after acquired resistance to cetuximab. Six kinases were also up-regulated, including MET, RET, MST1, PDK4, KHK and DAPK1. Eight cell surface receptors were up-regulated, including MET, RET, GHR, IL1R1, IL6R, SMO, GFRA1 and GFRA2. Twelve growth factors and cytokines were up-regulated, including CCL16, CCL19, CCL21, CXCL12, FGF21, GDF2, GREM2, IGF1, IGF2, INHBC, INHBE and NRG1. Among these genes, MET and RET are members of the RTK (Receptor tyrosine kinase) family (40), the same as EGFR which is the target of cetuximab. Amplification of MET gene has been reported to lead to acquired resistance to cetuximab (21, 22). RET (41) and ESR1 (42, 43) were reported to correlate with endocrine resistance in breast cancer. SMO gene amplification was associated with resistance to EGFR TKIs in human lung cancer (44). NGR1 was reported to provide resistance to MEK inhibitors in metastatic uveal melanoma (45). Our results suggested that these up-regulated kinases, cytokines and cell surface receptors may play roles in acquired resistance to cetuximab and that the inhibitors or drugs targeting these proteins may sensitize CRC to cetuximab treatment.
A literature search was also conducted for all 699 up-regulated genes (see Materials and methods). Twenty-one genes have been reported to lead to drug resistance in cancers (Figure 3D, Supplementary Table IV). Fifty-six genes have been shown to correlate with drug resistance, sixty-two genes are known cancer genes and 171 genes have been reported to be associated with cancer (Figure 3D, Supplementary Table III). This result showed that nearly half (296/699=42.3%, Supplementary Table III) of the up-regulated genes are known drug resistance or cancer associated genes. The rest of the genes may also play roles in drug resistance or cancer development and are worth further validation.
Differentially expressed lncRNAs after acquired resistance to Cetuximab. Fifty-three lncRNAs were differentially expressed between biopsies of prior treatment and after acquired resistance (25 up-regulated and 28 down-regulated, Supplementary Table III). The change folds of up-regulated lncRNAs were much greater than those of down-regulated lncRNAs (10.82±1.15 vs. 4.97±0.32, p<0.001, Mann-Whitney U-test). The top two significantly up-regulated lncRNA were H19 [fold change (FC)=16.7, adjusted p<0.001] and HULC (FC=12.5, adjusted p<0.001, Supplementary Table III). Up-regulation of H19 was reported to be associated with drug resistance in human hepatocellular carcinoma cells (46). Up-regulation of HULC was reported to promote the progression of hepatocellular carcinoma (47) and CRC (48). Two down-regulated lncRNAs MALAT1 (FC=3.7, adjusted p=0.005) and GAS5 (FC=3.3, adjusted p=0.047, Supplementary Table III) were reported to be associated with drug resistance. Down-regulation of MALAT1 was observed in vincristine-resistant acute lymphoblastic leukemia (49). Down-regulation of GAS5 leads to trastuzumab resistance in breast cancer (50) and was reported to be associated with cisplatin resistance in non-small cell lung cancer (NSCLC) (51). Our results suggest that these differentially expressed lncRNAs may also play roles in resistance to cetuximab in mCRC.
Interestingly, more lncRNAs are down-regulated in acquired resistance samples even though down-regulated genes were significantly less than up-regulated genes (p<0.001, one-sided Fisher's Exact Test, Supplementary Table V). This result indicates that high expression of these down-regulated lncRNAs may play important roles in sensitizing CRC to cetuximab treatment.
Potential miRNA regulatory network and competitive endogenous RNAs associated with Cetuximab resistance. Twenty mature miRNAs were significantly up-regulated (>3 folds) and nine mature miRNAs were significantly down-regulated (>3 folds) when resistance to cetuximab occurred (Figure 4A, Supplementary Table VI). The 5’ and 3’ cleavage products (denoted as -5p and -3p in the names of mature miRNAs) of four miRNA precursors were both up-regulated in biopsies after acquired resistance, including mir-885, mir-122, mir-483, and mir-139. (Supplementary Table VI). Interestingly, miR-885-5p was reported to be up-regulated in non-small cell lung cancer cell resistance to gemcitabine (52), and was up-regulated in liver metastasis specimens of CRC patients (53). miR-885-5p was the most up-regulated miRNA in lymphovascular invasion carcinoid tumors compared with tumors without invasion (54). Even more interestingly, miR-885-5p was detected in serum. High serum miR-885-5p expression independently predicted prognosis and metastasis in CRC (55). These results suggest that the significantly up- or down-regulated miRNAs may potentially become biomarkers for cetuximab resistance.
We further built the miRNA-mRNA negative regulatory network among differentially expressed miRNAs and mRNAs (Figure 4B, C, Supplementary Figure 1). Although down-regulated miRNAs were much less in number than up-regulated miRNAs (9 vs. 20), the target mRNAs of the down-regulated miRNAs were much more than those of the up-regulated miRNAs (Average target mRNA number: 35.22±22.16 vs. 5.53±3.45, p=0.004, t-test). These results suggest that the down-regulated miRNAs may play more important roles in resistance to cetuximab in mCRC. Up-regulation of the down-regulated miRNAs might sensitize CRC to cetuximab treatment.
Competitive endogenous RNA (ceRNA) is a pair of RNAs, which have the same miRNA response element (MRE) and may competing for the same endogenous miRNAs, and their expression changes in the same direction (56, 57). Based on this assumption, we predicted the ceRNA network among differentially expressed mRNAs and lncRNAs (Figure 4D). Seven lncRNAs and 32 mRNAs formed the ceRNA network. H19, the top significantly up-regulated lncRNAs, had the most potentially competitive mRNAs. The other 6 lncRNAs had 1 to 8 potentially competitive mRNAs. Some lncRNAs and mRNAs with known functions in cancer were involved in the network. For example, lncRNA H19, an imprinted gene, plays an important role in mammalian development (58) and has been reported to be related to development, metastasis and drug-resistance of various tumors (59-61). LncRNA Gas5, a tumor suppressor, has been correlated with drug resistance (62, 63). MMP9, a member of the MMP family, plays an important role in early progression of tumor and may promote proliferation, adhesion, migration and angiogenesis (64-66). CDKN2A (P16) is a known tumor suppressor gene (67-69). WIF1 is known to inhibit the Wnt protein by interacting with Frizzled, and then inhibit Wnt/β-catenin signaling transduction (70-72). The competitive relationship between these lncRNAs and mRNAs may exert functions in tumor resistance to cetuximab.

Analysis of differentially expressed genes after acquired resistance to cetuximab. (A) Heatmap of 835 differentially expressed genes between 2 groups prior to treatment and after acquired resistance. (B) The results of the gene functional enrichment analysis of 699 up-regulated protein-coding genes. Top panel shows the top 5 enriched KEGG pathways, and bottom panel shows the top 5 enriched biological processes. (C) Subcellular components and location of 26 specific genes, which code for cytokine, kinase, and cell surface receptors, among up-regulated genes. (D) Pie chart of categories of up-regulated genes identified by literature search.
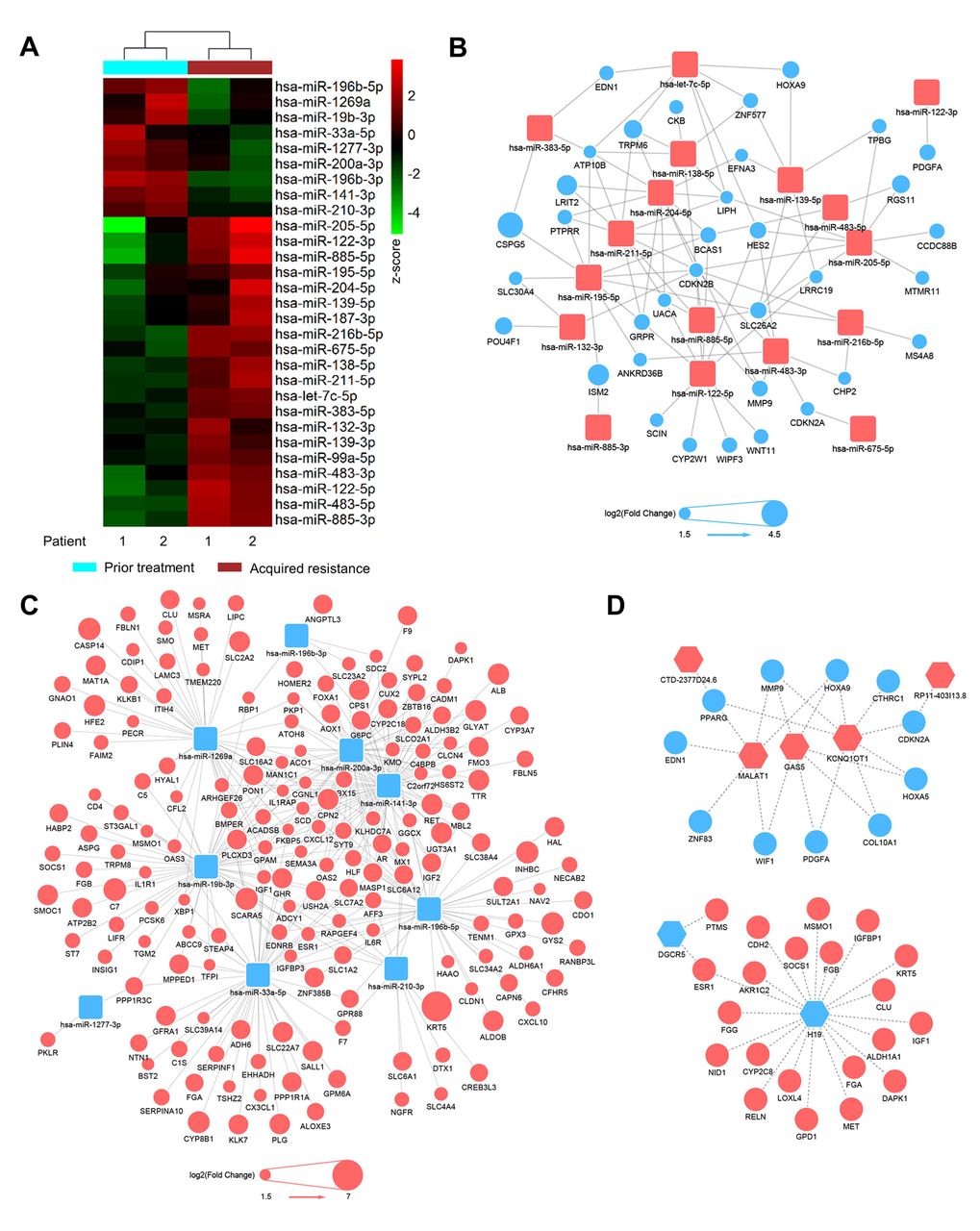
Integrative analysis of differentially expressed miRNAs, mRNAs and lncRNAs identified potential regulatory networks. (A) Heatmap of 29 differentially expressed miRNAs between 2 groups prior to treatment and after acquired resistance. (B and C) Predicted miRNA-mRNA negative regulatory network among differentially expressed miRNAs and mRNAs. Yellow squares represent up-regulated miRNAs (B) and down-regulated miRNAs (C). Circles represent down-regulated (blue in B) and up-regulated (red in C) mRNAs, and circle sizes are proportional to fold changes. (D) Predicted lncRNA-mRNA ceRNA regulatory network among differentially expressed lncRNAs and mRNAs. Yellow squares represent down-regulated (left panel) and up-regulated lncRNAs (right panel). Circles represent up-regulated (red in left panel) and down-regulated (blue in right panel) mRNAs.
Discussion
Acquired resistance to cetuximab widely occurs in the clinic. However, since paired biopsies prior to treatment and after acquired resistance from mCRC patients can rarely be obtained, global transcriptome alterations of paired biopsies are still unknown. We obtained four paired biopsy samples from two liver mCRCs, prior treatment with cetuximab and 5-FOLOX and after acquired resistance. By using high-throughput RNA and small RNA sequencing technology, we delineated global transcriptome changes when resistance occurred. Differential expression analysis, miRNA regulatory network and ceRNA network analysis suggested that some protein-coding genes, lncRNAs and miRNAs may be biomarkers and may play roles in the acquired resistance to cetuximab in mCRC. Our results provide clues for further studies of the molecular mechanisms of acquired resistance to cetuximab.
Cetuximab targets EGFR on the cell membrane, which is a member of the RTK family. The mutations or amplifications of several RTK family genes, including KRAS, NRAS, HER2 and MET, have been reported to result in acquired resistance to cetuximab (19-23). In our analysis, another RTK family member, RET, was significantly up-regulated in the biopsies of acquired resistance. Furthermore, three miRNAs miR-196b-5p, miR-141-3p and miR-200a-3p predicted to target RET mRNA were down-regulated in the biopsies of acquired resistance. RET has been reported to be related to drug resistance to endocrine therapy (73). Our results suggest that up-regulation of RET might also cause cetuximab resistance in mCRC.
Twenty-nine miRNAs were significantly up- or down-regulated in the biopsies of acquired resistance. MiRNAs are small molecules, ~22 nt in length. Some miRNAs can be detected in serum, for example, miR-885-5p. In our analysis, miR-885-5p was up-regulated in acquired resistance samples. It was reported that high serum miR-885-5p expression independently predicted prognosis and metastasis in CRC (55). These results suggest that miR-885-5p might be a serum biomarker of acquired resistance to cetuximab.
The functions and mechanisms of miRNAs and lncRNAs in acquired resistance are largely unknown. By constructing miRNA-mRNA regulatory networks and lncRNA-mRNA ceRNA networks, we predicted potential regulatory mechanisms for miRNAs and lncRNAs. For example, several miRNAs such as miR-141-3p and miR-1269a might contribute to sensitizing CRC to cetuximab treatment by inhibiting the genes that drive acquired resistance. LncRNAs such as H19 and MALAT1 might regulate critical genes that drive or inhibit resistance as competitive endogenous RNAs. This information provides clues for investigating the roles and mechanisms of miRNAs and lncRNAs in resistance to cetuximab.
Taken together, we depicted global transcriptome alterations between paired biopsy samples prior to treatment and after acquired resistance from two liver mCRCs treated with cetuximab and 5-FOLOX. To our knowledge, this is the first transcriptome profiling for paired biopsies of prior treatment and acquired resistance to cetuximab. The conclusion is preliminary due to the small sample size. Nonetheless, our results still provide clues for subsequent studies on the biomarkers and molecular mechanisms of cetuximab resistance.
Conclusion
Our study contributes to deciphering the molecular mechanisms of acquired resistance to cetuximab.
Acknowledgements
The Authors would like to thank all the medical and ancillary staff at the Cancer Center and the patients for consenting to participate. The Authors also thank Yun Shao and Yanhong Tai of the Department of Pathology for assistance with the preparation and assessment of formalin-fixed paraffin-embedded tumor samples, Gong-Jie Li of the Department of Radiology for assistance with radiological response evaluation and Tao Li and Xin Pan for their helpful discussions.
Footnotes
↵* These Authors contributed equally to this work.
Authors' Contributions
J. X. and X.Y. conceived the study; W.R., Z.L. and X.Y. wrote the manuscript; Z.L. and W.R. performed the transcriptome analysis with the help of S.H., Y.C., J.Z. and J.W.; Y.C., Y. W., Z. T. and T. L. conducted the clinical sample preparation and high-throughput sequencing. X. Y. and J. X. revised the manuscript. All authors reviewed the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare no competing financial interests.
Funding
This work was supported by National Key R&D Program of China (Grant No. 2017YFC0908300 to X. Ying), the China National High Technology Research and Development Program (No. 2014AA020604 to X. Ying), the National Natural Science Foundation of China Project (No. 81573458 to J. Xu), and the National Natural Science Foundation of China (Grant No. 81703006 to T. Li).
- Received February 17, 2019.
- Revision received April 5, 2019.
- Accepted April 8, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}