


Abstract
Molecular classifications of several malignancies are already accepted and applied in clinical practice. For head and neck squamous cell carcinomas (HNSCCs) there exist few and controversial data regarding their stratification on distinct groups or sub-groups and thus, none of them are validated as useful tools for diagnosis and therapy. Starting from the highly expressed markers in HNSCC (epidermal growth factor receptor, keratin 5 and E cadherin) we proposed to identify distinct HNSCC sub-groups with a potential impact on prognosis and therapy. Complex analysis of immunohistochemical expression for six surrogate markers (EGFR, p53, Bcl2, CD117, keratin 5 and E-cadherin) defined three distinct sub-classes amongst EGFR-positive cases, based on the association and differential expression of p53 and Bcl2 (EGFR+/p53−/bcl2−, EGFR+/p53+/bcl2− and EGFR+/p53+/bcl2+). Amongst them, only the EGFR+/p53+/bcl2− sub-class showed significant correlations with grade and TNM parameters. Keratin 5-positive cases were grouped in a special “basal like” group with a particular sub-class rich in CD117+/p63+ cells also highly expressing EGFR. Presence of K5+/CD117+/p63+ cells was correlated with all TNM staging parameters defining a particular sub-class with high aggressiveness and particular behavior. Our data sustain EGFR as the key player in the pathogenesis of HNSCCs, but its diagnostic value may be improved by association with other prognostic or therapeutic markers. We herein defined two distinct HNSCCs groups (EGFR+ and K5+) with several sub-classes, identifiable by the additional assessment of p53, Bcl2 and CD117.
Understanding of head and neck squamous cell carcinomas (HNSCCs) molecular biology is far from beeing elucidated. Despite continuous research in the field by more or less complicated molecular techniques, such as immunohistochemistry, microarrays, gene expression profiles or assessment of miRNA (1-4), presently there exists no validated and accepted molecular classification of HNSCCs. Recent data in the literature define six distinct molecular sub-types (immunoreactive, inflammatory, human papilloma virus (HPV)-like, classical, hypoxia associated, and mesenchymal) based, mainly on meta-analysis of their main biological characteristics and de-regulated signaling pathways (5). The current classification omitted one of the previously described sub-class of HNSCC, the basal type (6, 7), known to be one of the most aggressive phenotype for other cancer types as basal-like breast cancer (8).
Some of the articles published in the field of HNSCCs molecular classification attempted to classify such malignancies according to HPV involvement in the promotion of HNSCCs carcinogenesis (9, 10) suggesting a potential molecular signature of HPV on prognosis and therapy (11, 12). HPV is a recognized etiological factor in HNSCCs, but is not accepted to have a prognostic or therapeutic role, its impact on molecular differences among HNSCCs being still controversial. Moreover HPV association with other markers, as EGFR, failed to prove its involvement in EGFR mutation and targeted therapy resistance development (13, 14).
Compared to HPV, epidermal growth factor receptor (EGFR) is recognized to be overexpressed in up to 90% of HNSCCs cases (15) but its gene amplification is not found in more than 30% of cases (16).
Starting from the highly expressed markers in HNSCC (epidermal growth factor receptor, keratin 5 and E cadherin) we proposed to identify distinct HNSCC sub-groups with a potential impact on prognosis and therapy by applying a complex analysis of immunohistochemical expression for six surrogate markers (EGFR, p53, Bcl2, CD117, keratin 5 and E-cadherin). This emerges from previous data found in the literature on the molecular classification of HNSCCs most of them being exclusively based on genetic analysis, neglecting direct microscopic or immunohistochemical observations. None of the current reported gene analysis-based classifications have a certified impact on prognosis and therapy of HNSCCs.
Materials and Methods
We retrospectively assessed 42 cases of head and neck squamous cell carcinomas previously collected by surgery from patients with tumor masses developed on larynx (n=27), pharynx (n=12), and oral cavity (n=3). Paraffin-embedded specimens were selected for morphological evaluation and immunohistochemical assessement. Three-micrometer serial sections were obtained from each case. Initial histopathological evaluation on hematoxylin and eosin-stained slides (tumor type and grade) was followed by immunohistochemistry performed with a fully automated workflow system (Bond Max, Leica Microsystems, Milton Keynes, UK). Antibody selection was performed accordingly with markers proposed to be evaluated on HNSCC specimens, markers well-known to have a prognostic and/or therapeutic impact proved in other cancer types. This panel included p53 (clone DO7, Novocastra, Newcastle upon Tyne, UK), Epidermal Growth Factor Receptor (EGFR, Novocastra), Keratin 5 (K5), Bcl2 and E cadherin (E-cad). Aditionally, for K5+/EGFR+ cases we performed immunohistochemistry for co-localization of p63 with stem cell factor receptor (c-kit, CD117) to identify cells with a stem like potential. Immunohistochemistry used biotin-free visualization system (Bond Refine Detection System, DAB, Leica, Microsystems) and the final product was highlighted in brown, on nuclear (p53, p63), cytoplasmic (K5, CD117) and membrane (Bcl2, EGFR, Ecadherin) level of tumor cells. A co-localization evaluation of p53 and EGFR and p63 with Cd117 as well, were performed by using double immunostaining which additionally used a Bond Refine Detection System Red.
Based on the microscopic evaluation, we stratified HNSCCs according to the expression and co-localization of previous mentioned markers. Correlations between tumor grade, and TNM staging parameters were performed in order to evaluate the impact of our classification proposal on prognosis and therapy of HNSCC.
Results
All cases included in the study were squamous cell carcinomas with or without the presence of keratinization. A percent of 64.2% were localized at the laryngeal level while 28.5% came from different anatomical regions of the pharynx and 7.3% from oral cavity (tongue and salivary glands). Regarding tumor grade, 7.14% were classified as G1, 73.8% as G2 and 19% as G3. For selected cases, TNM staging parameters were evaluated and most cases were T3 (45.2%) and T2 (38%). Only one case was graded as T1 (2.3%) and six cases were T4 (14.5%). Regarding the N parameter, 64.28% of cases were graded as N1, 26.19% as N2 and 9.52% as N3. For 90.47% of cases M parameter was noted as M0, while in only 4 cases we observed M1 parameter.
Five markers with certified role in tumorigenesis, prognosis and therapy of various malignancies were selected to characterize HNSCC: p53, EGFR, Bcl2, E-cadherin and K5. A high variability in terms of number of cases and expression pattern was registered among cases as shown in Table I. When we performed a general evaluation of HNSCCs we obtained a significant correlation between G and Bcl2 (p=0.033), M parameter to EGFR expression (p=0.039) as well as between p53 and EGFR (p=0.001).
Half of the total number of cases expressed p53. All p53-positive cases also co-expressed EGFR while not all EGFR-positive cases were positive for p53. No significant differences of other markers between p53-positive and -negative groups were detected.
Regarding EGFR in HNSCC, this marker showed the highest percentage of positive cases amongst markers selected for evaluation. A percent of 85.71% of cases had moderate or intense positive reaction for EGFR. About 55% of EGFR-positive cases also co-expressed p53. Inside the EGFR-positive sub-group, we observed the highest number of K5-positive cases (K5-EGFR co-expression found in 61% of cases). In this sub-group, a special attention was given. It is well-known that in normal stratified epithelium from the head and neck region, EGFR expression is restricted to basal cells layer. In HNSCC, EGFR overexpression was associated with the presence of K5. This aspect suggested to us the possibility that this particular HNSCC sub-group could have derived from basal cells by activation of factors with stem-like potential. Thus, we considered it would be useful to characterize this sub-group by assessment of p63 and stem cell factor receptor (CD117, c-kit). The co-expression of p63 and CD117 was found in 75% of K5+/EGFR+ cases (42.85% of total cases included in the present study). Based on these findings we can define a special “basal-like” HNSCC subgroup characterized as K5+/p63+/CD117+/EGFR+. For this sub-group, a significant correlation was highlighted between G and p63 expression (p=0.01) and also for T which significantly correlated with CD117 expression (p=0.04) as well as with CD117/p63 co-expression (p=0.04).
Despite the low number of EGFR-negative cases found in the present study, they represented a special sub-group with the highest negativity for other markers. Except K5 (found positive in half of cases) and E cadherin also, no positivity for other markers has been detected for EGFR-negative cases. Due to the limited number of such cases, no other statistical or correlative appreciation regarding this group can be performed at the moment.
Procentual stratification of HNSCCs based on co-expression of surrogate markers assessed in the present study.
As shown in Table II, Bcl2 and p53 seem to be specific for EGFR-positive sub-group being absent in EGFR-negative sub-group. Based on p53 and Bcl2 expression in EGFR+ cases sub-group exclusively, we were able to define three distinct subclasses: EGFR+/p53−/bcl2−, EGFR+/p53+/bcl2− and EGFR+/p53+/bcl2+. The assessment of G and TNM staging parameters for these 3 sub-classes revealed that, for EGFR+/p53+/bcl2−, the N parameter showed significant correlation with EGFR (p=0.04) and also with CD117+/p63+ coexpression (p=0.04). A classification of EGFR-positive cases can be seen in Figure 1.
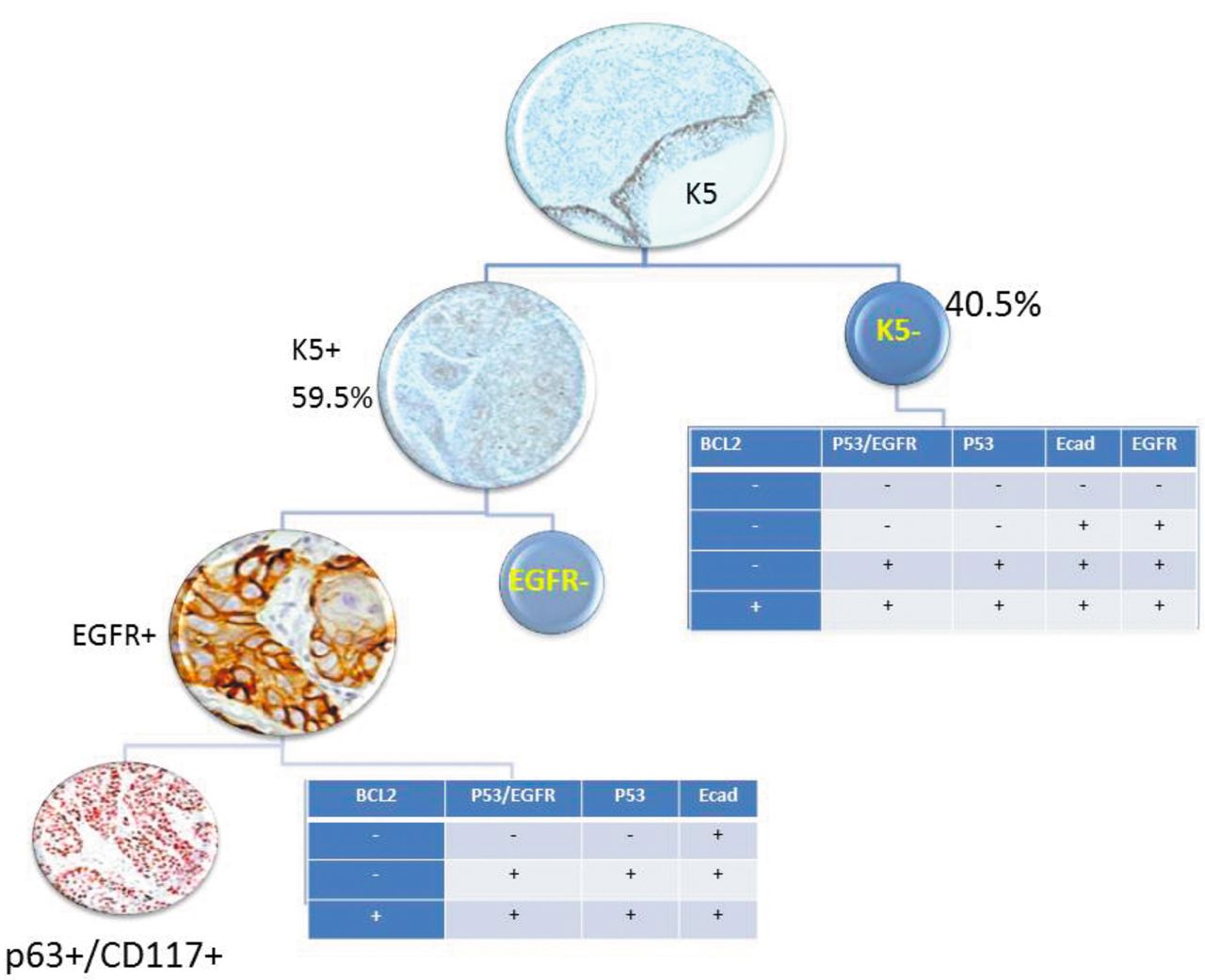
Keratin 5 was positive in 59.5% of cases. The most frequent co-expressions were observed for K5 with EGFR and CD117/p63. For these cases, an inverse significant correlation was observed between T parameter and p53/EGFR co-expression (p=−0.03) and a positive significant correlation between T parameter and the presence of CD117+/p63+ cells (p=0.01). The N parameter showed a significant correlation with Bcl2 (p=0.04). An inverse correlation has been obtained between M parameter and p53/EGFR co-expressing cells (p=−0.02) and a normal one between M and Bcl2 (p=0.01). P53/EGFR co-expression seems to be strongly associated with the presence of CD117+/p63+ cells in K5+ group of HNSCC (p=0.04). No K5−/EGFR+ cases has been detected in our study. All these data are summarized in Figure 2.
Percent of Bcl2-positive cases of HNSCC was relatively low (26.2%) but all of them had an intense EGFR co-expression. EGFR-positive cases represented a heterogeneous group. Inside this group we identified five distinct sub-groups based on differential expression of selected markers as shown in Table II. A quarter of EGFR-positive cases did not express any other marker while over 40% co-expressed 3 or 4 markers together with EGFR. These cases were predominantly G2 or G3, and classified as T2, 3 and N2 or N3 parameters of TNM staging.
Next marker which showed a high positivity in HNSCC was E cadherin. For all positive cases, E cadherin has a normal membrane pattern, with no aberrant expression observed among cases. For these cases an inverse correlation was obtained between tumor grade and K5 (p=−0.05) and also Bcl2 (p=−0.04).
Differences between EGFR+ and EGFR− groups regarding expression of p53 and Bcl2.
Discussion
Identification of prognostic and therapeutic markers in malignancies represents the “gold standard” in the multimodal evaluation of tumors, with these factors being responsible for revealing an optimal overall survival and disease-free survival.
Various types of malignancies with heterogeneous origins (arising from any component of the head and neck region as the lip, tongue, larynx, pharynx) are included in a larger group, generally defined as HNSCCs. The lack of the well-defined prognostic and therapeutic factors characterize the relatively common cancers included in the HNSCCs group as tumors with high morbidity, high mortality and limited therapy outside surgery, standard cytotoxic chemotherapy and radiation (17).
HNSCCs evaluation has mainly focused on the HPV involvement in their tumorigenesis (18, 19) and directed to EGFR assessment as a potential therapeutic target for such tumors (20-22). Unfortunately, most previous studies evaluated HPV or EGFR separately both in experimental and clinical studies (23, 24, 25), and this could be a possible reason for the inconsistent results with low prognostic and therapeutic impact for HNSCCs (26, 27, 28) until now. Because of HPV involvement more as an etiologic than prognostic factor in HNSCCs, our study ignored HPV presence, as it was not the primary focus of our study and, we studied EGFR correlated with other prognostic and therapeutic factors.
Recent studies applied panels of markers for a more complete characterization of HNSCCs most probably due to the stringent need of a molecular classification with a real impact on patient survival and life quality.
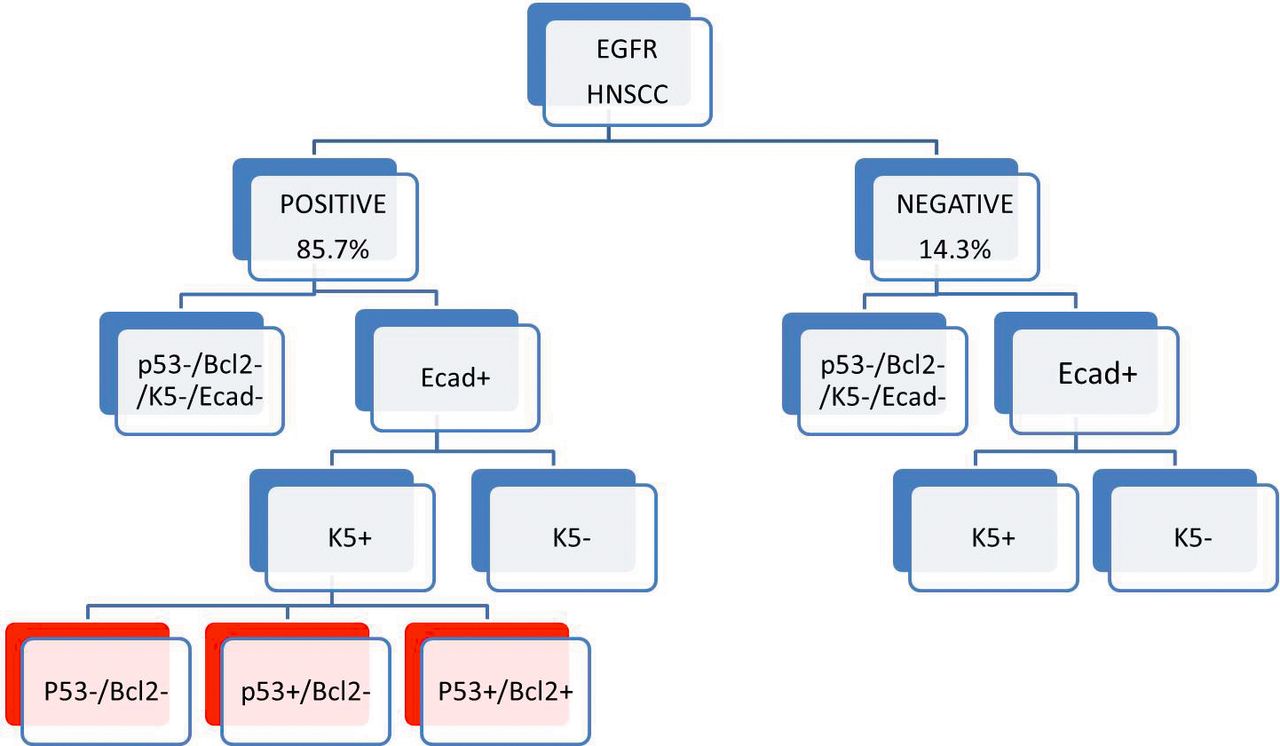
HNSCCs classification starting from EGFR expression. It has been shown that the EGFR+ group includes three sub-groups defined by the expression of p53 and Bcl2.
Most of HNSCC research has focused on the evaluation of other intermediate steps of the intracellular pathways mainly involving tumor suppressor and apoptosis genes together with growth factors and their correspondent receptors in malignant tissue (29, 30, 31, 32) and adjacent normal tissue (33). Moreover, genomic analysis is more frequently used for HNSCCs mapping and this seems to have an impact on prognosis and therapeutic response (34, 35). But not all pathology laboratories are able to perform genomic analysis of HNSCCs.
Thus, immunohistochemistry remains one of the most reliable methods to assess protein expression of surrogate markers in different tumors, including HNSCCs. Previous molecular classification stratified HNSCCs in four main subgroups. Shortly after first description of two clinically distinct sub-classes based on gene expression patterns (36), Chung and coworkers (using a similar protocol previously used by Perou for breast cancer) (37) defined in 2004 four sub-classes of HNSCCs (EGFR-pathway signature, a mesenchymal-enriched subtype, a normal epithelium-like subtype, and a sub-type with high levels of antioxidant enzymes) (38). More than ten years later, Walter confirmed Chung's classification by introducing p63 and SOX2 in this evaluation. Despite these efforts, the findings have not been replicated, no model systems have been proposed, and the etiology of the subtypes is obscure (7).
All proposed classification included EGFR expression assessement. Our results were in concordance with previous studies, showing that EGFR was positive in a high number of cases, the percentage being over 80%. But, compared to previous data, we stratified EGFR-positive cases according to the expression of K5, p53 and Bcl2. When we analyzed K5+/EGFR+ cases, we identified a sub-class characterized by p53 and Bcl2 expression which was specific for this K5+/EGFR+ sub-group and not found for EGFR-negative cases.

Keratin 5 expression impact on HNSCCs classification. A K5+/EGFR+/p63/CD117+ sub-group has been identified as a distinct class of HNSCCs.
The p53 protein is involved in the maintenance of the cellular integrity after DNA damage. Mutation of the p53 gene is an early event in HNSCCs carcinogenesis (38), and p53 loss was associated with a metastatic phenotype in a mouse model of head and neck cancer (39).
Controversial data have been published regarding EGFR and p53 co-expression. Some authors concluded that, p53 loss stimulate metastasis development (39), while others indicated that p53 may enhance sensitivity to EGFR inhibitors and radiation via induction of cell-cycle arrest, apoptosis, and DNA damage repair, suggesting a central role of p53 in the development of acquired resistance to EGFR inhibitors and prompt consideration to apply p53 restoration strategies in future clinical trials that combine EGFR inhibitors and radiation (40). Identification of p53/EGFR co-expression in more than half of EGFR+ cases may define a HNSCCs sub-class more sensitive to anti-EGFR therapy and with low potential to aquisite resistance to anti-EGFR therapy. For this group we identified for the EGFR+/p53+/Bcl2-sub-class a significant correlation with N parameter of TNM staging and also with the presence of CD117/p63-positive cells. Based on this observation we can speculate that, by targeting EGFR, we would be able to reduce nodal spreading of tumor cells with a stem-like potential characterized by CD117/p63 co-expression. Importance of p53/EGFR co-expression in HNSCCs was scattered highlighted in the literature, most of the studies being performed on a small number of cases from a limited geographic area (41, 42). Our findings are concordant with those reported by Keller and Hama (43, 44) regarding EGFR correlation with nodal metastases and grade but these previous studies did not assess the p53 impact on EGFR+ HNSCCs cases and also did not state that p53 expression is restricted to EGFR+ cases, being absent for EGFR− group.
Recently, Bcl2 has been extensively studied in HNSCCs regarding its association as a biomarker and clinical outcomes of patients (45, 46), but the results seem to contradict the findings in some older studies (47, 48), and produced additional reports that contradict each other for EGFR (49, 50). A recent study published by Kim in 2014 (51) pointed-out that, overexpression of a mutant p53 could down-regulate Bcl-2 at both the protein and mRNA levels based on previous scattered data (52), such that studies looking at Bcl-2 as a potential biomarker may need to account for the p53 status of tumors. Our study identified three distinct sub-classes of EGFR+ HNSCCs based on the association of p53 and Bcl2 specifically expressed inside this group. For most cases the presence of p53 seems to down-regulate Bcl2 expression (EGFR+/p53+/Bcl2−) in the present study, but two more sub-classes including a lesser number of cases has been identified (EGFR+/p53+/Bcl2−, EGFR+/p53+/Bcl2−). Further studies including a higher number of such cases will be needed to elucidate the prognostic and therapeutic role of these associations.
Another particular group identified in the present study had as main marker keratin 5 expression (K5). This group was characterized by the highest number of significant direct or inverse correlations with all TNM staging parameters. About 40% of K5+/EGFR+ cases contained CD117+/p63+ cells suggesting a basal-like phenotype rich in cells with stem potential, most probably with origin in the basal layer of stratified epithelium, cells which may have a more aggressive phenotype by the presence of CD117. Previous studies recognized a cancer stem cells (CSCs) compartment in HNSCCs frequently identified at the invasive front of the tumors and characterized by Oct4, Sox2, and CD44 (53, 54, 55). Almost all these studies reported the involvement of HGF/c-met pathway in the renewal and surviving of CSCs in HNSCCs.
CD117 (c-kit) was previously used as unique marker to differentiate between salivary gland adenoid cystic carcinoma and other tumor types with head and neck origin. Association between p63 and CD117 has not been previously used to characterize HNSCCs. This association was reported to be associated with a poor overall survival in patients with triple-negative breast cancer (56), but its prognostic and therapeutic impact in HNSCCs is still an unresolved problem. Assessement of EGFR+/K5+ HNSCCs for the expression of CD117 could define a special therapeutic group eligible for combined anti-EGFR and anti-CD117 therapy.
Conclusion
Our results sustain the re-classification of HNSCCs by use of markers with prognostic and therapeutic impact in other tumor entities. Starting from EGFR and K5 (highly expressed in HNSCCs) we defined two particular phenotypes with prognostic and therapeutic impact.
Acknowledgements
This work was supported by P III-C1-PCFI/2014-2015 granted by “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania.
- Received September 4, 2015.
- Revision received September 30, 2015.
- Accepted October 19, 2015.
- Copyright© 2016, International Institute of Anticancer Research (Dr. John G. Delinasios), All rights reserved




{kind=link}
{kind=link}