


Abstract
Background/Aim: MicroRNAs (miRs) play an important role in the regulation of cancer-related processes and are promising candidates for cancer biomarkers. The aim of the study was to evaluate the association of response to anti-EGFR monoclonal antibodies (mAbs) with selected miR expression profiles, including miR-125b, let-7c, miR-99a, miR-17, miR-143 and miR-145 in metastatic colorectal cancer (mCRC) patients. Patients and Methods: This retrospective study included 46 patients with mCRC harbouring wild-type RAS gene treated with cetuximab or panitumumab combined with chemotherapy in first- or second-line therapy. The miR expression was assessed using qRT-PCR. Results: Down-regulation of miR-125b and let-7c and up-regulation of miR-17 were found in the tumour tissue (p=0.0226, p=0.0040, p<0.0001). Objective response rate (ORR) was associated with up-regulation of miR-125b (p=0.0005). Disease control rate (DCR) was associated with up-regulation of miR-125b and let-7c (p=0.0383 and p=0.0255) and down-regulation of miR-17 (p=0.0464). MiR-125b showed correlation with progression-free and overall survival (p=0.055 and p=0.006). Conclusion: The results show that up-regulation of miR-125b is associated with higher ORR and DCR and longer survival; let-7c up-regulation and miR-17 down-regulation are associated with higher DCR in mCRC patients treated with anti-EGFR mAbs.
Colorectal cancer (CRC) is one of the most common malignancies whose incidence has been increasing in developed countries (1). Clinical trials have provided evidence for the efficacy and safety of monoclonal antibodies (mAbs) targeting the epidermal growth factor receptor (EGFR) represented by cetuximab and panitumumab, in the treatment of patients with metastatic CRC (mCRC). Both agents have been widely used in mCRC patients with tumours harbouring a wild-type RAS gene. Despite the standard use of RAS gene mutations as effective biomarkers predictive of resistance to anti-EGFR mAbs, there is a large proportion of patients with tumours harbouring a wild-type RAS gene who obtain poor benefit from this systemic treatment (2-9). There is therefore an urgent need for novel complementary predictive and prognostic biomarkers.
MicroRNAs (miRs) are small non-coding RNAs, consisting of approximately 18-25 nucleotides that play an important role in the regulation of target gene expression. MiRs are involved in the regulation of key cancer-related processes including proliferation, differentiation, apoptosis, cell adhesion and angiogenesis (10). The role of miRs as biomarkers useful in diagnostics or prognostic estimation in cancer patients has been extensively studied.
The aim of the present study was to evaluate the association of a number of selected miR expression profiles with response to anti-EGFR mAbs in mCRC patients harbouring a wild-type RAS gene. The selected miRs included: miR-125b, let-7c, miR-99a, miR-17, miR-143 and miR-145.
Patients and Methods
Patients and treatment. The study included 46 patients with histologically confirmed mCRC who were treated with a combination of anti-EGFR mAbs (cetuximab or panitumumab) and chemotherapy as first- or second-line treatment between the years 2010 and 2019 at the Department of Oncology and Radiotherapeutics, Medical School and University Hospital in Pilsen, Czech Republic. The chemotherapy backbone consisted of the following regimens: fluorouracil and leucovorin in combination with oxaliplatin (FOLFOX), or with irinotecan (FOLFIRI). Panitumumab (Vectibix, Amgen Inc., Thousand Oaks, CA, USA) was administered in combination with chemotherapy, or as a single agent, in the standard approved dose (6.0 mg/kg every 14 days). Cetuximab (Erbitux, Merck & Co., Kenilworth, NJ, USA) was administered in combination with chemotherapy, or as a single agent, in the standard approved dose (initial dose 400 mg/m2, further doses 250 mg/m2 every 7 days). None of the patients had previously received anti-EGFR mAbs.
Clinical monitoring. Clinical data were obtained retrospectively from the hospital information system. Physical examination and routine laboratory tests were performed every two weeks; a computed tomography (CT) or positron emission tomography – (PET)-CT was performed every three months of the treatment. The objective tumour response was assessed by an experienced radiologist using Response Evaluation Criteria in Solid Tumours (RECIST) version 1.1 in terms of: complete response (CR), partial response (PR), stable disease (SD) and progressive disease (PD); objective response rate (ORR) included patients achieving CR and PR; disease control rate (DCR) included those achieving CR, PR and SD (11).
The study protocol was approved by the independent Ethics Committee of the Medical School and University Hospital in Pilsen and complied with the International Ethical Guidelines for Biomedical Research Involving Human Subjects, Good Clinical Practice guidelines, the Declaration of Helsinki, and local laws.
Assessment of miR expression. The total RNA from tumour tissue samples and macroscopically healthy adjacent non-tumour colon mucosa was isolated using TRI Reagent® RT (MRC, Cincinnati, OH, USA), following the manufacturer's protocol. The total RNA concentration was measured by Qubit RNA HS Assay Kit (ThermoFisher Scientific, Waltham, MA, USA) and all samples were diluted to 2 ng/μl before reverse transcription. For the assessment of miR expression, gene-specific TaqMan assays (ThermoFisher Scientific) were used. The targets of the analysis were: hsa-miR-125b-5p (assay ID 000449), hsa-miR-17-5p (assay ID 002308), hsa-let-7c-5p (assay ID 000379), hsa-miR-145-5p (assay ID 002278), hsa-miR-143-3p (assay ID 002249) and hsa-miR-99a-5p (assay ID 000435). hsa-miR-16-5p (assay ID 000391) and hsa-miR-345-5p (assay ID 002186) were chosen as reference genes based on our previous experience (12). TaqMan® MicroRNA Reverse Transcription Kit (ThermoFisher Scientific) was used for the separate reverse transcription of individual genes using target specific primers from corresponding TaqMan Assays. The relative expression of microRNAs was measured in duplicates in 10 μl reactions using the CFX96 real-time PCR system (Bio-Rad, Hercules, CA, USA) with TaqMan® Universal Master Mix II, with UNG (ThermoFisher Scientific). The following amplification parameters were used: 2 min at 50°C and 10 min at 95°C, followed by 45 cycles of 15 s at 95°C and 1 min at 60°C. All reactions were tested for nonspecific signals.
Statistical analysis. Standard frequency tables and descriptive statistics were used to characterize the patient group. Changes of miR expression levels in tumour tissue (relative to adjacent non-tumour tissue) were expressed in -ΔΔCt values and because of their mostly normal distribution (as reviewed in histograms and using a Shapiro-Wilk test) were analysed using parametric methods. Expression of the miR-143/miR-145 cluster was determined as an arithmetic mean of -ΔΔCt values for miR-143 and miR-145, and was analysed analogically to the other miR expression levels. A one sample t-test against a zero reference was used to test for significant up- or down-regulation. Differences in the level of change in miR expression between pairs of treatment response groups (objective response (CR or PR) achieved/not achieved, and disease control achieved (CR, PR or SD)/not achieved) were tested for significance using a two-sample t-test.
Progression-free survival (PFS) was determined from the date of anti-EGFR therapy initiation until the date of first documented progression, or death. Overall survival (OS) was determined from the date of anti-EGFR therapy initiation until the date of death, regardless of its cause. Patients who had not progressed or died were censored at the date of their last follow-up. Median survival times were calculated from the Kaplan-Meier estimates of survival functions using linear interpolation between the nearest complete observations. The median follow-up was estimated from OS data using the inverse Kaplan-Meier method. Significance of associations between miR expression change and survival times was assessed using a univariable Cox proportional hazards model. In order to visualize these associations and detect possible non-proportional ones, significant or borderline results were reviewed using automated stratification. In this procedure, a threshold (cut-off) miR expression change value was determined by an automated optimization process finding the threshold that provided the lowest Cox-Mantel p-value in the two-sample Kaplan-Meier analysis, which was finally verified using a Gehan-Wilcoxon test.
All reported p-values are two-tailed and the level of statistical significance was set at α=0.05. Statistical processing and testing was performed in a STATISTICA data analysis software system (StatSoft, Inc.2013, Version 12, www.statsoft.com) and Matlab (2019b, MathWorks Inc., Natick, MA, USA).
Results
Patient characteristics. The study included 46 mCRC patients. The median age at anti-EGFR therapy initiation was 63.6 (range=37.3-82.5). Thirty-four (73.9%) patients were males, 30 (65.2%) had the primary tumour localized in the colon, 27 (58.7%) had synchronous metastatic disease, 36 (78.3%) received the anti-EGFR mAbs-containing regimen as first-line therapy. Twenty-five (54.3%) patients were treated with panitumumab and 21 (45.7%) patients were treated with cetuximab. The baseline patient characteristics are summarized in Table I. The median PFS of the whole cohort was 8.9 months (95% CI=7.0-12.26) and the median OS was 26.4 months (20.1-39.2). Median follow-up time was 61.7 months. ORR and DCR in the whole cohort were 54.3% (95% CI=39.9-68.1%) and 78.3% (63.9-88.1%), respectively.
Baseline characteristics of included patients.
Expression of miR-125b, let-7c, miR-99a, miR-17, miR-143 and miR-145 in the tumour tissue. Low tumour expression of miR-125b and let-7c in comparison with adjacent non-tumour tissue was found in 27 out of 42 (64.3%) and 30 out of 43 (69.8%) patients, respectively (p=0.0226 and p=0.0040, respectively). High tumour expression of miR-17 in comparison to adjacent non-tumour tissue was observed in 33 out of 39 (84.6%) patients (p<0.0001). There were no significant differences in the expression of miR-99a, miR-143, miR-145 or the whole miR-143/miR-145 cluster between tumour and adjacent non-tumour tissue (p=0.1851, p=0.5376, p=0.3862 and p=0.2392, respectively). The differential expression levels of assessed miRs are shown in Figure 1.

The differential expression levels of assessed miRs between tumour and adjacent non-tumour tissues.
Association of miR-125b, let-7c, miR-99a, miR-17, miR-143 and miR-145 with response to anti-EGFR mAbs. ORR (CR+PR) was significantly associated with up-regulation of miR-125b (p=0.0005) (Figure 2A), while the relative expression levels of let-7c, miR-99a, miR-17, miR-143, miR-145 and the whole miR-143/miR-145 cluster were not associated with ORR (p=0.1418, p=0.1565, p=0.6419, p=0.9015, p=0.7799 and p=0.8553, respectively). DCR (CR+PR+SD) was significantly associated with up-regulation of miR-125b and let-7c (p=0.0383 and p=0.0255, respectively) and down-regulation of miR-17 (p=0.0464) (Figure 2B, C and D), while the relative expression levels of miR-99a, miR-143, miR-145 and the whole miR-143/miR-145 cluster were not associated with DCR (p=0.1211, p=0.9706, p=0.7399 and p=0.8580, respectively).
Association of miR-125b, let-7c, miR-99a, miR-17, miR-143 and miR-145 with PFS and OS. The results of the univariable Cox proportional hazards model suggested a possible association with PFS and OS only for miR-125b dysregulation, however, without confirming statistical significance [p=0.1389 with hazard rate (HR) of 0.849 per unit of -ΔΔCt value for PFS, and p=0.0680 with HR of 0.771 for OS]. The remaining miRs showed no indication of being associated with PFS or OS (p>0.2 for all). After further investigation using automated optimization of stratification threshold, miR-125b showed strong separation between long- and short-surviving patients at a threshold value of -2.17 (i.e. 4.5-fold decrease of miR-125b levels in tumour tissue) (Figure 3). Contrastingly, its performance for other threshold values was mediocre.
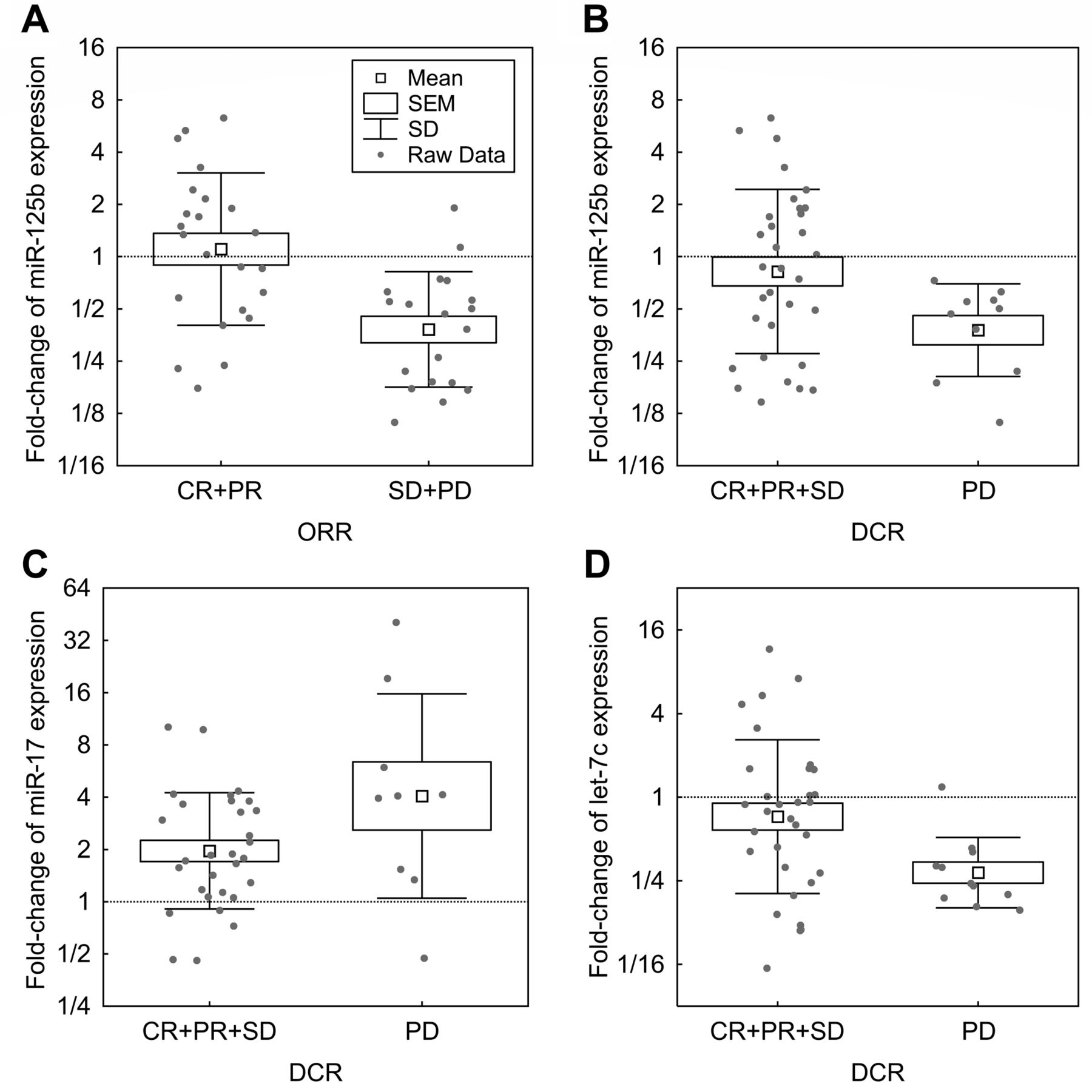
The association of differential expression levels of miR-125b with objective response (A), miR-125b with disease control (B), miR-17 with disease control (C) and let-7c with disease control (D).
Discussion
The treatment of mCRC has been markedly changing in recent years with the introduction of targeted therapies leading to improvements in patient survival. Prognostic and predictive biomarkers play a crucial role in the management of cancer as they help clinicians use the optimal treatment strategy for each individual patient. Our data suggest that down-regulation of miR-125b and let-7c, as well as up-regulation of miR-17, are associated with a poor response to systemic therapy based on anti-EGFR mAbs. We, therefore, suggest that these miRs are promising candidates for predictive biomarkers.

Progression-free survival (PFS) (A) and overall survival (OS) (B) according to miR-125b differential expression levels using automated optimization of stratification threshold value of 4.5-fold decrease of miR-125b levels in tumour tissue.
In the field of mCRC, RAS gene mutations, including KRAS and NRAS mutations, represent well-established predictive biomarkers. Nevertheless, a large proportion of mCRC patients with tumours harbouring wild-type RAS gene derive poor benefit from systemic treatment based on anti-EGFR mAbs.
The basic function of miRs is regulation of expression of target protein coding genes by binding to their specific messenger RNA (mRNA), leading to mRNA degradation and subsequently to inhibition of protein translation (13). Each miR achieves functional specificity by targeting a core network of genes involved in multiple signaling pathways (14). Therefore, miRs may act as oncogenes or tumour suppressor genes and their dysregulation (i.e. up-regulation or down-regulation) is common in cancer. In the field of cancer treatment, miRs can serve as potential targets for the systemic therapy and also they are regarded as promising candidates for novel cancer biomarkers (15-17). As diagnostic biomarkers, circulating and urinary miRs have the potential to be non-invasive and cheap diagnostic tools. In terms of prognostication, there is a hope that miR signatures, eventually combined with other genetic or clinical factors, will be able to more precisely stage and subtype cancers according to the prognosis of patients and/or response to the systemic therapies. In the future, they could be used as valuable predictive biomarkers playing a key role in the treatment individualisation within the concept of personalised oncology.
In the present study, we focused on the association of the dysregulations of miR-125b, let-7c, miR-99a, miR-17, miR-143 and miR-145 with the outcome of mCRC patients harbouring a wild-type RAS gene who had been treated with anti-EGFR mAbs combined with standard chemotherapy as first- or second-line therapy. The selection of investigated miRs was based on a literature search.
MiR-125b is a member of the miR-125 family, which is known to play a crucial role in many cancer-related processes including proliferation, cell differentiation and apoptosis (18). The targeting of multiple genes involved in the process of initiation and progression of cancer by miR-125b has been described in the literature and miR-125b dysregulation is commonly seen in many cancers. Interestingly, miR-125b targets both tumour suppressor genes and oncogenes, leading to its up- or down-regulation having distinct effects, which seem to be dependent on specific tumour type (18). Down-regulation of miR-125b has been described in breast cancer, non-small-cell lung cancer, oesophageal squamous cell cancer, bladder cancer, thyroid cancer, melanoma, hepatocellular cancer, ovarian cancer, osteosarcoma, chondrosarcoma, and CRC. Its up-regulation has been reported in retinoblastoma, nasopharyngeal cancer, glioblastoma and certain leukemias (18, 19). Among others, miR-125b targets the p53 tumour suppressor gene: a key regulator of apoptosis (20). Additionally, it has been demonstrated that miR-125b targets several other apoptosis regulators, such as PUMA and BAK1 as well as cell cycle regulators, including cyclin C (20). Consequently, in tumours characterised by miR-125b up-regulation, miR-125b predominantly acts as an oncogene, leading to the blocking of apoptosis and causing stimulation of proliferation. On the other hand, miR-125b also targets genes encoding human epidermal growth factor receptor (HER) 2 and 3, which represent important oncogenic signalling molecules that are up-regulated in several cancers, typically in breast cancer (21). In these tumours, miR-125b down-regulation causes increased HER2/3 signalling involved in carcinogenesis and cancer progression and miR-125b may predominantly act as a tumour suppressor. The role of miR-125b dysregulation in CRC is poorly understood, and its association with the outcome of patients treated with anti-EGFR targeted therapy is particularly unclear. In the present study, we observed significant down-regulation of miR-125b in the CRC tissue compared to the adjacent non-tumour tissue. This is in agreement with a study previously reported by Chen and Xu, who further suggested that DNA hypermethylation may be involved in down-regulation of miR-125a and miR-125b in CRC (22). We found a significantly lower ORR and DCR as well as a shorter PFS and OS for patients with miR-125b down-regulation. These results are in line with a previous study conducted by Capuzzo et al. that included 183 mCRC patients from two independent cohorts treated with anti-EGFR mAbs (23). In our study, however, after taking into account the limited sample size, the significant differences in PFS and OS were obtained following an optimization process that found the threshold for the lowest p-value in a Kaplan-Meier analysis. This analysis showed a strong separation between long- and short-surviving patients using the optimised threshold value. Contrastingly, the results for other threshold values were mediocre, suggesting that its relationship to survival is nonlinear.
Let-7c is a member of the let-7 family including let-7a, let-7b, let-7c, let-7d, let-7e, let-7f, let-7g, let-7i, miR-98 and miR-202 (24). Their main role is regulation of cell differentiation and proliferation, which they achieve by targeting a variety of signalling pathways (25). For instance, the let-7 family negatively regulates the expression of RAS as well as other oncogenes such as MYC, IGF1 and HMGA2, which represent critical regulators for the growth of CRC (26-28). Thus, the let-7 family members are widely viewed as tumour suppressors down-regulated in many cancers, including CRC (29). In our study, we found a significant down-regulation of let-7c in the CRC tissue compared to the adjacent non-tumour tissue, which is in agreement with Han et al.; whose study also shows correlation with poor survival (30). In the study by Cappuzzo et al., let-7c down-regulation was associated with a shorter OS but not with a shorter PFS or DCR in mCRC patients treated with anti-EGFR mAbs (23). Even though we did not observe a significant correlation with survival - a fact that could be attributed to the limited patient cohort, we found a significantly lower DCR for patients with let-7c down-regulation in our study.
MiR-99a participates in the regulation of epithelial–to–mesenchymal transition (EMT), which has been recognised as one of the key cancer-related processes (31). MiR-99a has been demonstrated as a tumour suppressor in a variety of cancers, and miR-99a down-regulation in CRC has previously been reported (32). Moreover, the conclusions of a retrospective study including 78 mCRC patients have suggested that miR-99a dysregulation could be a predictor of a patient's response to chemotherapy (33). Nevertheless, in our study the survival, ORR or DCR, of the mCRC patients treated with chemotherapy combined with anti-EGFR mAbs showed no association with miR-99a expression.
MiR-17 is a member of the miR-17-92 cluster, which expresses six miR precursors and plays an important role in carcinogenesis (34). In CRC, it is mainly involved in the regulation of EMT and proliferation via targeting CYP7B1 and SIK 1 genes, respectively (35, 36). Additionally, several other potential target genes for miR-17 have been suggested (36). In the present study, we demonstrated a significant miR-17 up-regulation in the tumour in comparison with adjacent non-tumour tissue, which is consistent with the findings of Huang et al. and Lai et al. (36, 37). It has, furthermore, been suggested that miR-17 up-regulation is associated with poor prognosis of cancer patients in a meta-analysis conducted by Huang et al. (38). Even though it has been reported that miR-17 up-regulation is associated with a short OS in CRC patients, the data from patients with metastatic stage treated with systemic therapies are limited and its prognostic or predictive role within this group remains unclear. We observed a correlation of DCR with miR-17 down-regulation. The difference however, was on the edge of statistical significance, and was marginally statistically significant. We did not find any significant difference in PFS or OS that was associated with miR-17 dysregulation.
MiR-143 and miR-145 form a cluster that plays a role in the regulation of multiple cell processes such as proliferation, apoptosis, invasion, differentiation and angiogenesis (39). These miRs are able to suppress cancer progression by targeting numerous oncogenes, indicating that they have a tumour-suppressive role (39). Although the down-regulation of the miR-143/miR-145 cluster has been described in several cancer types, inconsistent results have been reported in CRC (40-44). We did not find any significant dysregulations in miR-143 or miR-145, nor in the whole miR-143/miR-145 cluster, when tumour tissue was compared with adjacent non-tumour tissue. Thus, we did not confirm the results of several previously reported studies with limited sample sizes (40-43). Our results are nevertheless in line with those obtained from a large cohort of CRC clinical specimens studied by Schetter et al. (44). Furthermore, the data on the prognostic or predictive role of these miRs are conflicting. Drebber et al. reported that patients with advanced rectal cancer and a low post-therapeutic expression of miR-145 had a significantly worse response to neoadjuvant chemo-radiotherapy (45); similarly, Zhang et al. observed serum miR-145 as one of the 17 miRs predicting chemosensitivity in CRC patients (46). On the other hand, Schee et al. did not find any significant associations between miR-145 dysregulation and metastasis-free or overall survival (47). The results of our study show no significant association of outcome with the dysregulations of miR-143, miR-145, or the whole miR-143/miR-145 cluster.
The principal limitations of the present study are its retrospective design and the limited number of patients included, introducing a possible bias caused by the interindividual differences in various clinical parameters. Therefore, the results for PFS and OS were limited and the statistically significant difference was revealed only after optimization of the threshold, as mentioned above. Thus, we mainly focussed on the analysis of ORR and DCR, which allowed us to compare responders and non-responders. The present study furthermore lacked a control cohort not treated with anti-EGFR mAbs, and, therefore, whether the observed miR dysregulations may be a predictive factor exclusively for anti-EGFR-based targeted therapy cannot be concluded with certainty. This issue should be addressed in a future prospective randomised clinical trial. Nevertheless, this is the first study focusing on the role of selected miRs including miR-125b, let-7c, miR-99a, miR-17, miR-143 and miR-145 in mCRC patients treated with anti-EGFR mAbs.
In conclusion, the results of the present retrospective study show that the up-regulation of miR-125b and let-7c and the down-regulation of miR-17 are associated with good response to the combination of anti-EGFR mAbs and chemotherapy as a first- or second-line therapy. Our data suggest that these three miRs may serve as promising predictive biomarkers. We have not demonstrated an association between the dysregulation of miR-99a, miR-143 and miR-145 and patients' outcome. A future prospective study with a large patient cohort should be conducted in order to confirm these results.
Acknowledgements
The Authors would like to thank all patients voluntarily taking part in the study. This study was supported by the project “Center of Clinical and Experimental Liver Surgery”, UNCE/MED/006, by the National Sustainability Program I (NPU I) Nr. LO1503 provided by the Ministry of Education Youth and Sports of the Czech Republic and by the Charles University Research Fund (Progres Q39), by the European Regional Development Fund-Project „Application of Modern Technologies in Medicine and Industry” (No. CZ.02.1.01/0.0/0.0/17_048/0007280), by the Ministry of Health, Czech Republic - conceptual development of research organization (University Hospital in Pilsen - FNPl, 00669806). and by the European Union's Horizon 2020 research and innovation programme under grant agreement N°856620.
Footnotes
Authors' Contributions
OF designed the study and wrote the manuscript with support from OS, PH, VL, JB, OV, RK, OT, JF, DM and PP. VL, OV and JB collected tissue samples. PP and DM performed laboratory analyses. PH performed statistical analyses.
This article is freely accessible online.
Conflicts of Interest
OF received honoraria from Roche, GSK and Pfizer for consultations and lectures unrelated to this project. JF has received honoraria from Astra Zeneca, Roche and Novartis for consultations and lectures unrelated to this project. OS, PH, VL, OV, JB, RK, OT, DM and PP declare that they have no actual or potential conflict of interest including any financial, personal or other relationships with other people or organizations that could inappropriately influence this work.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available due to patient data security but are available from the corresponding author on reasonable request.
- Received May 31, 2020.
- Revision received June 21, 2020.
- Accepted June 23, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.