


Abstract
The goal of this study was to investigate the expression of some metalloendopeptidases in squamous cell carcinomas of the oropharynx as well as its relation to histological differentiation, staging of disease, and prognosis. Paraffin blocks from 21 primary tumors were obtained from archives of the Department of Pathology, Paulista Medical School, Federal University of Sao Paulo, UNIFESP/EPM. Immunohistochemistry was used to detect the expression of EP24.15 and EP24.16 by means of tissue microarrays. Expression of EP24.15 or EP24.16 was not correlated with the stage of disease, histopathological grading or recurrence in squamous cell carcinomas of the oropharynx. In summary, our results support the notion that EP24.15 and EP24.16 are expressed in carcinoma of the oropharynx; however, these do not appear to be suitable biomarkers for histological grading, disease stage or recurrence as depicted by tissue microarrays and immunohistochemistry.
Head and neck neoplasms are the sixth most common type of cancer worldwide (1). About 90% of these tumors are squamous cell carcinoma (SCC) and the oropharynx is a site commonly involved (2). This neoplasm arises from accumulated damage to genes that control cellular proliferation, invasion, motility and survival (3). These genetic alterations most often occur as the result of exposure to tobacco, alcohol and other carcinogens. In particular, prolonged exposure to these agents results in irreversible damage to the DNA of the oropharyngeal mucosa which leads to alterations in the coding and regulatory regions of cell cycle regulatory genes. To date, a few studies have demonstrated the expression of such genes in SCC of the oropharynx, especially in relation to the histopathological grading, stage of disease and recurrence (4, 5).
Acumulating evidence suggests that metalloendopeptidases 24.15 (EP24.15; thimet oligopeptidase) and 24.16 (EP24.16; neurolysin) play important roles in endothelium-mediated vasoregulation (6). These enzymes show the characteristic zinc binding motif HExxH and belong to the M3 metallopeptidase family (7-9). They are able to inactivate some polypeptides of less than 17 residues (10).
EP24.15 was first proposed to participate in peptide catabolism based on its ability to hydrolyze the Phe5-Ser6 bond of bradykinin (11). EP24.16 was first identified and characterized on the basis of its capacity to cleave neurotensin (12). EP24.15 and EP24.16 have been demonstrated by biochemical and immunohistochemical methods to be widely distributed in mammalian tissues (13,14). Both are highly concentrated in the brain and are reportedly enriched in areas containing putative peptide substrates (15).
Although both EP24.15 and EP24.16 are primarily soluble, cytosolic enzymes, membrane-associated forms have been demonstrated in a number of cell types. For example, Crack et al. (16) have detected immunoreactive EP24.15 on the extracellular membrane of intact corticotrophic tumor cells, whereas EP24.16 has been localized to the plasma membrane in neurons, both in vivo (17, 18) and in vitro (19), as well as in human kidney cells transfected with the peptidase (20). Given that neither enzyme possesses a transmembrane domain, the exact mechanism of its association with the membrane is not understood. Furthermore, the expression of EP24.15 or EP24.16 in the context of the neoplasias has not been explored.
As a result, the aim of the present study was to investigate the expression of EP24.15 and EP24.16 in SCC of the oropharynx and to correlate their expression with histopathological grading, stage of the disease and recurrence by means of immunohistochemistry.
Materials and Methods
Cases. A total of 21 cases of SCC of the oropharynx were obtained from the archives Department of Pathology Federal University of Sao Paulo, UNIFESP/EPM. The mean of age was 52 years-old being 18 men and 3 women. Ethical approval for this study was granted by the local Ethics Committee (Resolution no. 196 of the National Health Council). Diagnoses from histological typing of oral lesions and normal mucosa were made by two of the authors (DAR and GF). All cases were included prior to any treatment.
Tissue microarray method (TMA). Histological sections of 4 μm were cut from each block from biopsy samples and stained by hematoxylineosin (H.E.). The slides were evaluated for diagnostic confirmation and re-evaluation of the histopathological findings, including the selection of sites for the removal of cylindrical cores used in TMA block construction. All tumors were classified according to U.I.C.C. (2000) classification (21). TMA blocks were constructed using Beecher™ equipment (Beecher Instruments, Silver Spring, MD, USA) according to the manufacturer's instructions, in the following stages: i) The selected area in the respective paraffin block was marked; ii) A cylindrical core was created in the receptor block using the apparatus; iii) An 1 mm cylinder of tissue was extracted from the area of interest; ix) The cylindrical tissues obtained from the donnor block was transferred to the core in the receptor block; v) New core positions were created in the receptor block, separated such that a collection of tissue samples was created following the matrix arrangement; vi) The quality of the block was assessed before storing. To guarantee adhesion of the TMA block slices to the slides, an adhesive tape system (Instrumedics Inc, Hackensak, NJ, USA) was used.
Immunohistochemistry. Paraffin-embedded tissue blocks were used to cut 3 μm-thick sections. Hematoxylin and eosin staining was carried out and serial sections were used for immunostaining of EP24.15 and EP24.16 proteins. Immunohistochemical staining was performed using the avidin-biotin method. Briefly, slides were deparaffinized in xylene and hydrated in ethanol. For antigen retrieval, the sections were boiled in citrate buffer (2.94 g/l sodium citrate, pH 6.0) for 30 minutes and subsequently cooled to 30°C. Endogenous peroxidase activity was blocked by incubating the slides in methanol with 3% H2O2 for 20 minutes, followed by washing in phosphate-buffered saline (PBS; pH 7.4). The primary antibodies were diluted 1:200 for EP24.15 and EP24.16, (Santa Cruz, CA, USA) in 1% bovine serum albumin (BSA), and sections were incubated for 16 hours at 4°C. After washing in PBS, the sections were incubated with secondary biotinylated antibody for 30 minutes with peroxidase-streptavidin conjugate (LSAB-HRP, Dako, Denmark). The sections were washed in PBS (pH 7.4) and the proteins were visualized for light microscopy with 0.06% 3,3-diaminobenzidine tetrahydrochoride and 0.03% H2O2 in phosphate-citrate buffer (Sigma, St. Louis, USA). Sections were counterstained with hematoxylin for 3 minutes. Positive controls were represented by mammary tissue. Negative controls were made by eliminating the primary antibody.
Data analysis. The presence of tumor tissue was confirmed previously in each core. Immunostaining was scored by two trained independent observers without prior knowledge of the clinicopathological parameters. Discordant cases were reviewed and agreed upon before data were statistically analyzed. For this purpose, tumor sections stained using immunohistochemistry were analyzed for the percentages of immunopositive cells under optical microscopy. A total of 1,000 epithelial cells were evaluated in 3-5 fields at ×400 magnification. All values were used as labeling indices. This protocol was established in previous studies conducted by our research group (22, 23).
Statistical analysis. Data from immunohistomemistry of p53, p16, p21, and Rb were evaluated by Kruskall-Wallis non-parametric test followed by post-hoc Dunn's test. Statistical analyses were performed with SPSS 15.0 for Windows and a p-value less than 0.05 was considered statistically significant.
Results
In this study, the variables analyzed to assess their influence on metalloendopeptidases were: size of tumour, presence of lymph node metastasis, stage (as depicted by the TNM system), grade of differentiation, and recurrence of disease.
A total of 21 cases were included in the present study. With respect to histological grading, six cases were categorized as well-differentiated type (type I), nine cases were categorized as moderate differentiated type (type II) and six cases were categorized as poorly differentiated type (type III). Regarding the TNM staging system, 15 cases were in advanced stage, i.e. type IV. A total of three cases were type III and three cases were type II. Finally, a total of eight cases experienced recurrence, whereas thirteen cases had not (for about four years and six months after initial diagnosis).
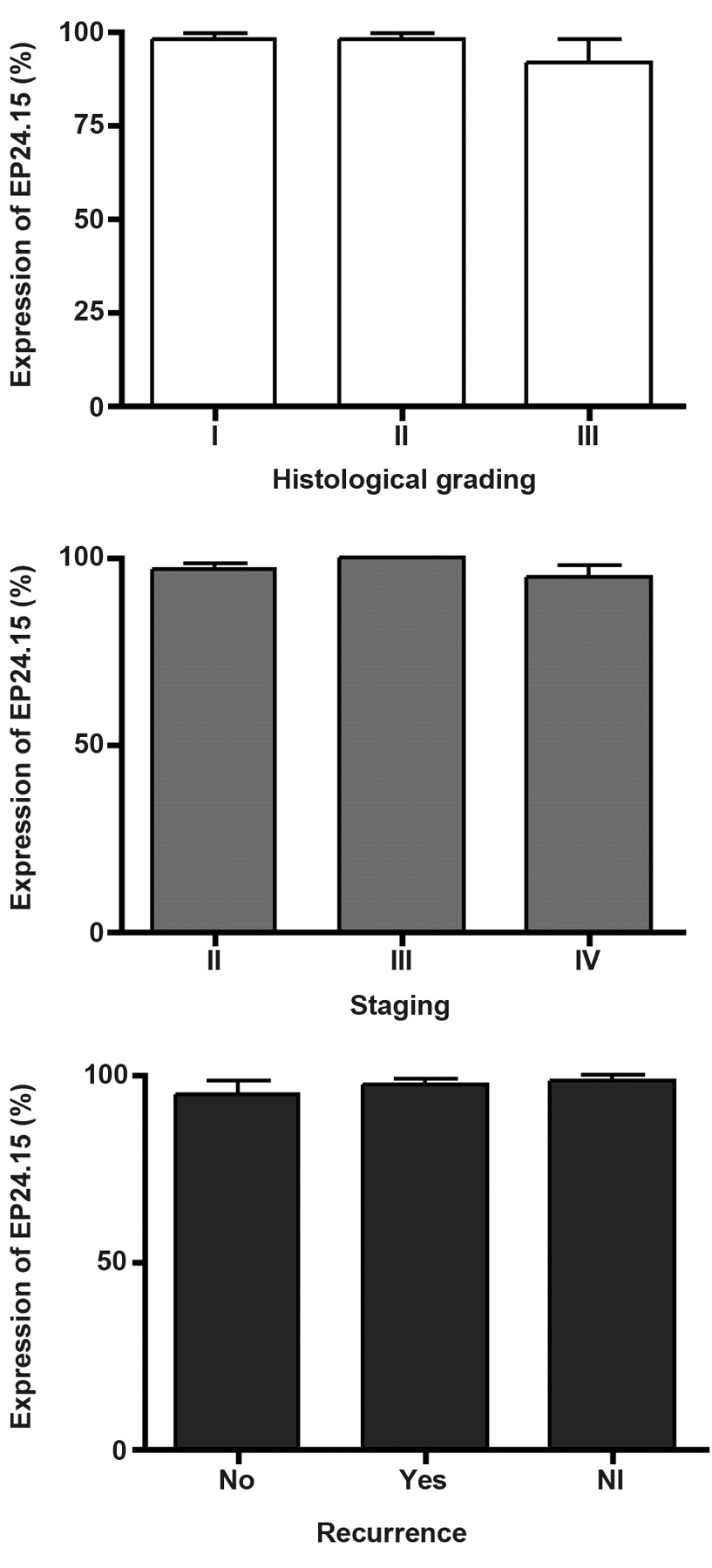
Immunohistochemical data revealed that EP24.15 protein immunoreactivity was considered high (>75% of positive cells) in SCC of the oropharynx and no significant differences were found when associated with histological grading, stage of the disease or recurrence (Figure 1). EP24.15 expression was predominantly cytoplasmic. A similar pattern was found for EP24.16 immunoexpression (Figure 2), i.e. strong expression, however, without statistically significant differences (p>0.05) when these parameters were considered (Figure 2).
Discussion
The aim of this study was to investigate the expression of EP24.15 and EP24.16 in SCC of the oropharynx by means of TMA and immunohistochemistry in order to predict their utility as putative biomarkers for the disease. These immmunomarkers were chosen because they play important roles in some solid tumors. To the best of our knowledge, this approach has not been addressed before.
High levels of EP24.15 activity have been localized, both catalytically and immunohistochemically, to the brain, pituitary, and testis, with lower levels in tissues such as the lung, liver, kidney, and spleen (24). Although primarily associated with the soluble fraction of tissue homogenates, subcellular fractionation of EP24.15 in rat brain shows that 20–25% of the total enzyme activity is associated with membrane fractions, including synaptosomes (25). Given the distribution of enzyme activity and its ability to degrade several bioactive peptides, Orlowski and colleagues (26) proposed a possible function in tissue metabolism. Our results demonstrated high levels of EP24.15 in oropharyngeal tumor cells for all case studies in this setting. The expression was not correlated with histological grading, recurrence of grade or differentation of the neoplasia. Taken as a whole, we assume that EP24.15 is present in SCC of the oropharynx, but the protein is not able to differentiate some tumor types. Further studies are necessary to elucidate this issue.
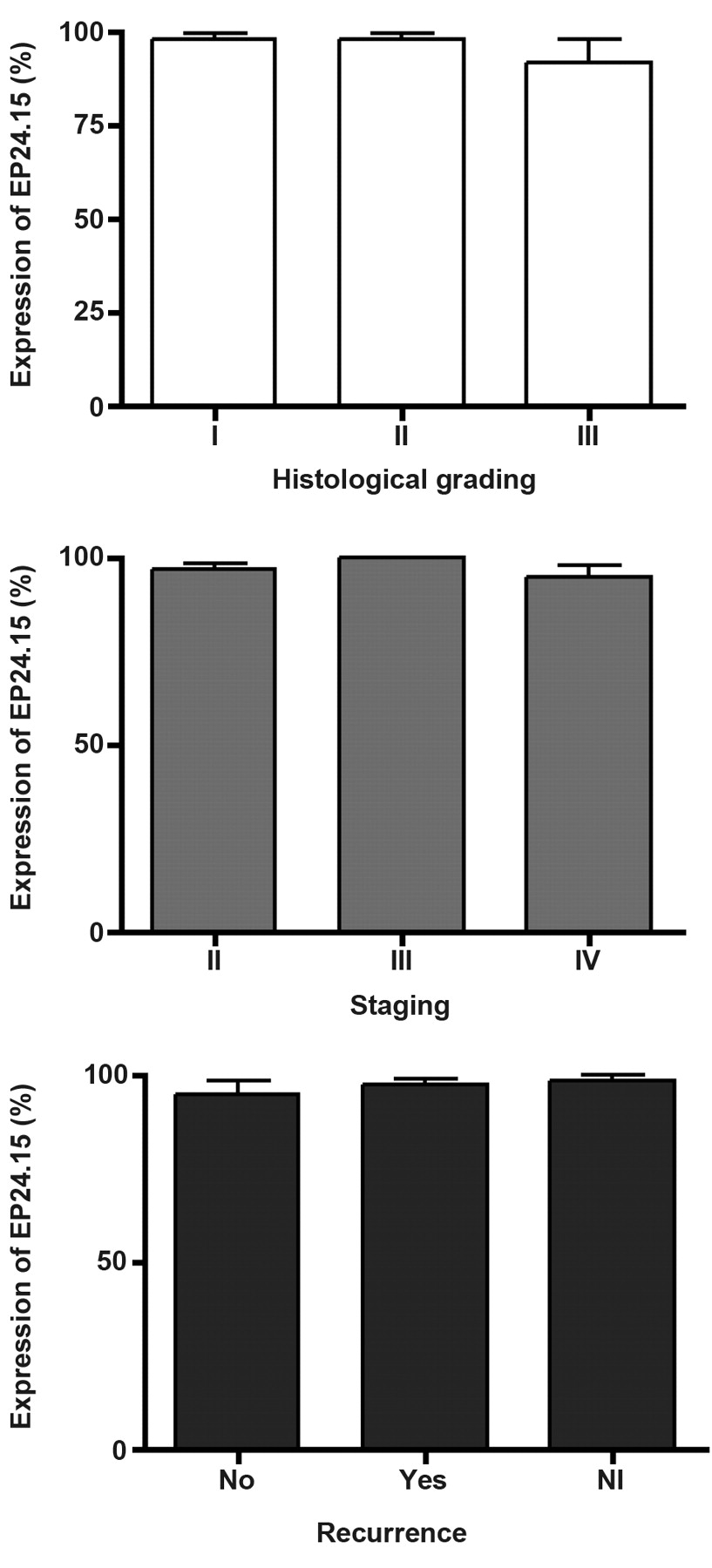
EP24.15 labelling index in squamous cell carcinomas of the oropharynx with respect to histological grading, stage of the disease (TNM system) and recurrence. Values are expressed as Mean±S.D. (n=21). NI: Cases Indetermined. p>0.05.

EP24.16 labelling index in squamous cell carcinomas of the oropharynx with respect to histological grading, stage of the disease (TNM system) and recurrence. Values are expressed as Mean±S.D. (n=21). NI: Cases Indetermined. p>0.05.
Regarding metalloendopeptidase 24.16 (neurolysin), it was originally purified and characterized from rat synaptic membranes (14), and later from tissues such as rat ileum and kidney (27, 28), on the basis of its ability to cleave neurotensin, generating the biologically inactive fragments. EP24.16 was shown to be distinct from other enzymes capable of cleaving neurotensin. Our findings revelaed that EP24.16 is present in tumor cells from SCC of the oropharynx without significant differences. These data are new, and, therefore difficult to discuss. Independent of biological mechanims involved in this phenomenon, this protein is also expressed in SCC of the oropharynx.
In summary, our results support the notion that EP24.15 and EP24.16 are expressed in carcinomas of the oropharynx, however, these do not appear to be suitable biomarkers for histological grading, disease stage or recurrence.
- Received July 24, 2011.
- Revision received September 24, 2011.
- Accepted September 26, 2011.
- Copyright© 2011 International Institute of Anticaner Research (Dr. John G. Delinassios), All rights reserved




{kind=link}
{kind=link}