


Abstract
Background/Aim: PTEN-loss and PIK3CA mutations have been addressed as markers of PI3K activation in breast cancer. We evaluated these markers in early high-risk breast cancer (EBC) focusing on PTEN immunohistochemistry (IHC) issues, particularly in HER2-positive disease. Materials and Methods: We examined PTEN-loss and PIK3CA mutations in 1265 EBC patients treated with adjuvant chemotherapy within two clinical trials. Two different methods for the evaluation of PTEN IHC were used, one upfront binary (loss; no-loss) and the other initially multi-scale allowing for the classification of “grey zone” tumors with low and very low PTEN protein expression. Results: PTEN-loss (33.4% and 22.1%, depending on the IHC method) and PIK3CA mutations (29.6%) were associated with ER/PgR/HER2-negative and ER/PgR-positive disease, respectively. Concordance of the two IHC methods was moderate (Cohen's kappa 0.624). PTEN-loss discrepancy and intra-tumor heterogeneity concerned “grey zone” tumors that were prevalent among HER2-positive cancers. PTEN-loss independently conferred higher risk for relapse and death. Compared to single PIK3CA mutations,single PTEN-loss was independently associated with increased risk for relapse and death. Depending on the evaluation method, in HER2-positive cancer, PTEN-loss was without- or of marginal unfavorable prognostic significance. Conclusion: In EBC, PTEN-loss is an independent predictor of poor outcome. When occurring singly, PTEN-loss and PIK3CA mutations have opposite prognostic impact. In HER2-positive disease, assessment of PTEN-loss by IHC appears unreliable and the marker is without clear prognostic significance.
- PTEN immunohistochemistry
- heterogeneity
- discordance
- PI3K pathway
- HER2-positive breast cancer
- adjuvant chemotherapy
- trastuzumab
The PI3K/PTEN/AKT axis operates within the PI3K/AKT/mTOR pathway as a key regulator of most cancer hallmarks. In this axis, PTEN (phosphatase and tensin homolog; gene on chromosome 10q23) is a tumor suppressor that dephosphorylates phosphatidylinositol-3,4,5-triphosphate into 4,5-biphosphate and thus deactivates the phosphatidylinositide-3-kinase (PI3K) [reviewed in (1-3)]. PTEN-loss and mutations in PIK3CA, the p110 catalytic subunit of PI3K, are linked to the activation of the PI3K pathway, which is targeted by diverse classes of specific and general inhibitors.
PTEN-loss in cancer occurs due to mutation, deletion or transcriptional inactivation (4). In breast cancer, PTEN-loss is infrequently based on PTEN genomic alterations (5), while it appears that decreased expression even without complete loss of this protein may be important for the biology of disease (6-8). The prevalence of PTEN-loss ranges from 4% to 63% across different studies, being more frequent in ER/PgR-negative and HER2-negative tumors (9-13). PTEN-loss has been associated with aggravating clinicopathological features (13, 14) and adverse prognosis in all stages of breast cancer (15). In patients with early HER2-positive disease who were treated with adjuvant chemotherapy in the pre-trastuzumab era, PTEN-loss has been reported as an adverse prognosticator (11) or without prognostic significance (16); in patients who received adjuvant trastuzumab, PTEN-loss had no clear prognostic significance in the BCIRG-006 trial (11) and in the NCCTG N9831 trial (17). As yet, inhibition of the PI3K pathway has been more successful in ER-positive/HER2-negative [reviewed in (1, 18, 19)], but not in HER2-positive disease, despite initial evidence linking PTEN-loss with intrinsic resistance to HER2-inhibition (20).
The objective of this study was to investigate the impact of PTEN-loss, individually and in combination with the PIK3CA mutational status on the outcome of patients with operable breast cancer who had received anthracycline-taxane-based adjuvant chemotherapy. Although PTEN-loss and no-loss are usually evaluated with immunohistochemistry (IHC), and despite efforts to standardize this method with respect to the biological implications of decreased PTEN protein expression levels (11), there is currently no standard method for the evaluation of this marker. This appears to be a major cause of inconsistent results with respect to PTEN-loss as a marker in breast cancer (13, 15, 17, 21, 22). To address this question, we applied two approaches for the evaluation of PTEN IHC and present the corresponding sets of results for comparison, focusing on HER2-positive disease.
Materials and Methods
PTEN status was examined in routinely processed tumor tissues (FFPE) from patients with operable breast cancer who had been treated with adjuvant anthracycline-taxane-based chemotherapy within the HE 10/05 (ACTRN-12610000151033) (23) and HE 10/08 (ACTRN-12615000161527) clinical trials by the Hellenic Cooperative Oncology Group (HeCOG) described in (24). Patients with HER2-positive and ER/PgR-positive disease had received trastuzumab and hormonotherapy, respectively, based on local pathology typing. All patients had submitted informed consent for the use of their biological material for research purposes. The study was approved by the Bioethics Committee of the Aristotle University of Thessaloniki School of Health Sciences, Faculty of Medicine (#77/10June2014) and by the Institutional Review Board of the Papageorgiou Hospital of Thessaloniki (#725/10May2013). The status of PIK3CA mutations and their impact on patient outcome were previously described for these patients (24, 25). All tumors were re-assessed centrally at the Laboratory of Molecular Oncology (MOL; Hellenic Foundation for Cancer Research/HeCOG/Aristotle University of Thessaloniki, Thessaloniki, Greece) for histology; construction of low-density tumor microarrays including 2×1 mm cores per tumor; assessment of the density per stromal area of tumor infiltrating lymphocytes (TILs) according to (26); construction of low-density tissue microarrays including at least 2×1 mm cores per tumor; clinical subtyping with IHC4 (ER/PgR/HER2/Ki-67) resulting in the 5 classical subtypes described in Table I, with Ki67 cut-off at 14% for distinguishing between Luminal A and B tumors (27); and, implementation of PTEN IHC. Local/central pathology typing was 88% concordant for ER/PgR and 88.6% for HER2 status. For this study, the central annotation of breast cancer subtypes was used.
PTEN IHC. IHC for PTEN protein (clone 6H2.1, DAKO, Glostrup, Denmark) was applied on 3 μm-thick TMA sections. Following deparaffinization and rehydration, IHC staining was performed in a Bond-Max™ autostainer (Leica Microsystems, Wetzlar, Germany) using Bond Polymer Refine detection kit (DS9800, Leica). The slides were incubated for 20 min with EDTA (pH 9.0) for antigen unmasking, and for one hour with the primary antibody (dilution 1:300).
PTEN stained TMA sections were centrally and simultaneously evaluated by two breast cancer expert pathologists (E.V., I.K.) for the intensity of staining (negative=0; weak=1+, intermediate=2+, strong=3+) in stromal and tumor cells. Simultaneous observation was necessary for eliminating the issue of inter-observer variability when scoring low intensity staining. Percentage values were recorded for all intensity levels separately for each core, blinded to the identity of each tumor. Tumors completely negative for PTEN without evaluable stroma or with PTEN negative stroma were excluded from the analysis. We finally evaluated 1257 tumors (Figure 1), and recorded values separately for each core. We applied two approaches for the evaluation of PTEN protein status:
Binary Approach A: Tumor cores were considered as PTEN-no-loss, if PTEN protein was expressed in the cytoplasm and/or nucleus of at least 10% of the tumor cells at intensities 2+ and 3+. For tumors with weak stromal staining, PTEN-no-loss was considered if more than 10% of tumor cells demonstrated intensity 1+. This classification, previously used by our Group (16), yielded a binary result for PTEN protein expression, loss and no-loss; here, the “loss” category in fact included completely negative and PTEN-low tumors.
Selected patient and tumor characteristics, in the entire cohort and by trial.
Multi-scale Approach B: A previously described detailed evaluation for PTEN staining was also applied (11). This approach yielded a 5-scale classification for tumor PTEN protein expression: completely negative=0; weaker than the weak stroma (very low PTEN expression)=1*; weak (low PTEN expression)=1+; intermediate=2+; and, strong=3+. Categories 1+, 2+, 3+ were classified as PTEN-no-loss.
Intra-tumor heterogeneity of PTEN protein expression was assessed in 923 tumors with preserved multiple cores. With the binary Approach A, tumors with a heterogeneous core evaluation, i.e., loss and no-loss in the available cores [123 out of 924 tumors evaluable for heterogeneity (13.4%)] were classified as PTEN no-loss. With multi-scale Approach B, tumors with a heterogeneous core evaluation, i.e., 0 vs. 1+, 2+, or 3+ [77 out of 923 tumors evaluable for heterogeneity (8.3%)] were classified as PTEN-loss. Category 1* was finally classified as PTEN no-loss.
Characteristic examples of PTEN IHC are shown in Figure 2A. As per the manufacturer, the antibody used detects PTEN protein in the cytoplasm and in the nucleus. Although cytoplasmic and nuclear PTEN may have different functions (2), in practice, on paraffin tissue sections, it is impossible to appropriately assess PTEN protein staining separately in the two cellular compartments.
For readability purposes, we present significant results with the binary Approach A in the main text and those with the multi-scale Approach B in the supplementary data (https://figshare.com/s/c10051be3947b26052fb).
PTEN and PIK3CA genotypes. PTEN amplicons covering the most frequently mutated regions of this gene based on COSMIC and on previous reports (4, 5) were included in the previously published panel used for targeted next generation sequencing (NGS) for these tumors (28): ex1, 89624138-89624312; 89624218-89624385; ex7, 89717547-89717720; 89717672-89717822; ex8, 89720761-89720934; 89720839-89721012; ex9, 89724991-89725119 (GRCh37 coordinates on chromosome 10). The method, the eligibility criteria, and the PIK3CA mutations (exons 9 and 20) obtained using the same panel have been previously described for an extended series including the present cohort (24). PTEN and PIK3CA genotypes were informative in 961 tumors (Figure 1). We also compared the variant allelic frequencies (VAFs) of the identified mutations, as a surrogate measure of their clonal [VAFs >25% (29)] presence in tumors.
Statistical analysis. Patients with unknown PTEN by IHC (N=8) were classified as PTEN-loss if PTEN was mutant. The derived PTEN status (Figure 1) corresponded to PTEN-loss by IHC and/or PTEN mutant; and, PTEN-no-loss by IHC only.
Disease-free (DFS) and overall survival (OS) were defined as the time (in months) from the date of diagnosis until event (progression or death from any cause) or, in the absence of event, until date of last contact. Deaths without prior registered progression were considered as events. The clinicopathological parameters studied in association with DFS/OS are shown in Table I. The study variables were: PIK3CA mutations; PTEN IHC; PTEN status; and, PTEN status/PIK3CA mutations. For multivariate analyses, we considered clinicopathological parameters (univariate cox p<0.10), centrally assessed subtypes, PIK3CA mutations and PTEN status (model 1) and the combined PTEN status/PIK3CA variable (model 2). The final models included variables remaining significant upon a backward selection process with a removal criterion of 0.15. All analyses were performed in the entire cohort and in patients with concordant local/central HER2-positive tumor status.
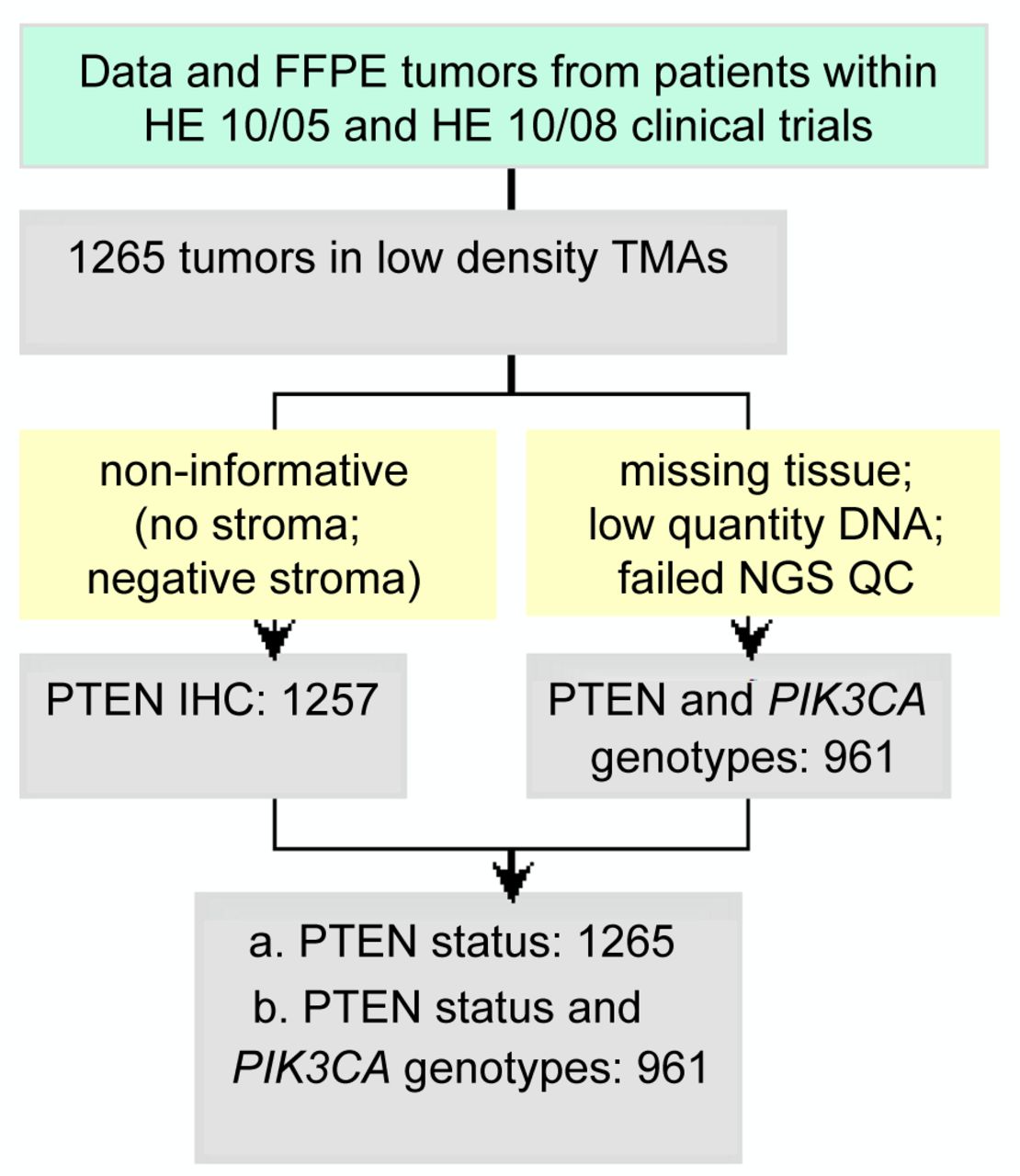
REMARK diagram. TMA: Tissue microarray; NGS: next generation sequencing; QC: quality control; IHC: immunohistochemistry. The final PTEN status corresponded to PTEN-loss by IHC and/or PTEN mutant; and, PTEN-no-loss by IHC only. This variable was assessed in 1265 tumors.
The statistical analyses were performed using the SAS software (SAS for Windows, version 9.3, SAS Institute Inc., Cary, NC, USA). Statistical significance was set at 2-sided p=0.05. Results of this study are presented according to reporting recommendations for tumor marker prognostic studies (30). This study is prospective-retrospective (31).
Results
Clinicopathological and treatment characteristics for the 1,265 patients in the entire cohort and in each trial are presented in Table I. Most patients were >50 y.o. and postmenopausal; the majority had low nodal burden disease and medium sized tumors, most of which were high-grade ductal carcinomas of non-specific type; 70.4% of the tumors were ER/PgR positive and 20.6% were HER2-positive.
Among the 1,257 tumors with informative PTEN IHC, PTEN-loss was classified in 415 (33%) with the binary Approach A and in 272 (21.6%) with the multi-scale Approach B. Concordance between the two approaches was 84.8% with a moderate agreement (Cohen's kappa 0.624). Discordance concerned tumors with low or very low PTEN protein expression (Figure 2A); out of 191 discordant tumors, 85.9% were classified as PTEN-loss with Approach A but as no PTEN-loss with Approach B (p<0.001). HER2-positive tumors were more frequently discordant than HER2-negative (p=0.010); again, PTEN discordance concerned low/very low PTEN expression in 18/18 HER2-enriched and in 22/24 Luminal-HER2 cases (p=0.005).

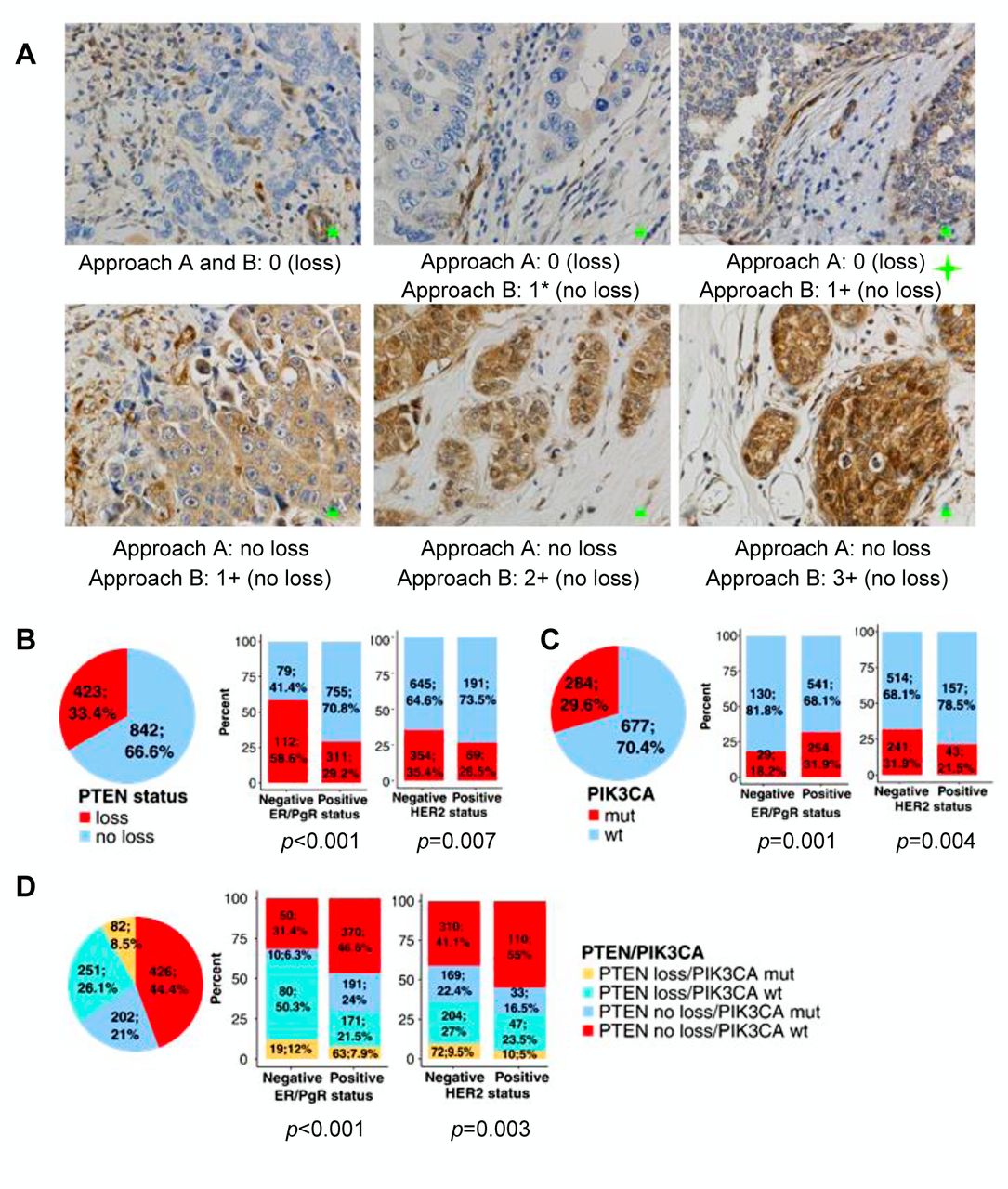
PTEN-loss and PIK3CA mutations in early high-risk breast tumors. A. Examples of PTEN immunohistochemistry (IHC) and evaluation of PTEN protein expression with the two approaches used in the present study. Discrepancies were observed for tumors expressing very low PTEN (pink star) or lower than the adjacent stroma and heterogeneous (green star). Green bars within microphotographs: 10 μm (original magnification: X400). Note that in tumors with 2+ and 3+ PTEN staining intensity, it is impossible to separately evaluate cytoplasmic and nuclear staining. B. Incidence of PTEN loss in the entire cohort and its association with tumor ER and HER2 status. C. Incidence of PIK3CA mutations, as in B. D. Combined PTEN/PIK3CA alterations in the entire cohort and their associations with ER and HER2 status. approximately 1 in 4 tumors with PTEN-loss having PIK3CA mutations, while 1 in 3 tumors with PIK3CA mutations had PTEN-loss. In B and D: PTEN status assessed by IHC in combination with pathogenic mutations in the gene. IHC Approach A.
Among 961 tumors with informative genotypes, the incidence of PTEN mutations was low, as expected for breast cancer (4, 5), unrelated to ER/PgR/HER2 status (32); 38 (4%) tumors had PTEN mutations most of which had previously been classified as pathogenic. PTEN mutations and PTEN IHC were mostly concordant with PTEN IHC Approach A (73.3% of the cases; p<0.001). We used the additional 8 pathogenic mutations to characterize PTEN-loss in cases without an informative IHC. The resulting PTEN status, informative for 1265 patients, was analyzed separately with the two IHC approaches (Figure 2B for Approach A).
PIK3CA mutations were present in 284/961 (29.6%) informative tumors (Figure 2C) and concerned missense changes in known hot-spots in exons 9 and mostly 20, as previously described (24, 25). PIK3CA mutations were present at higher frequencies (mean VAF=33.6%) compared to PTEN mutations (mean VAF=22.9%; p<0.001), in line with the reported clonal presence and driver role of PIK3CA mutations in breast cancer (5, 33).
Associations of PTEN with PIK3CA status and clinicopathologic parameters. PTEN-loss was significantly more frequent in ER/PgR-negative (58.6%) and in HER2-negative (50.6%) tumors (Figure 2B), while PIK3CA mutations showed the opposite distribution compared to PTEN-loss with respect to ER/PgR and HER2 status (Figure 2C). PTEN-loss was not mutually exclusive with PIK3CA mutations, although these two alterations did not tend to occur simultaneously (p=0.020). Among the 961 tumors informative for PTEN status and PIK3CA genotypes, 8.5% had simultaneous PTEN-loss and PIK3CA mutations, 26.1% had PTEN-loss only (single PTEN-loss), 21% PIK3CA mutations only (single PIK3CA), and the rest had none of these alterations (Figure 2D).
PTEN-loss was present in more than 50% of TNBC, in about 20% of HER2-enriched tumors, and at significantly lower rates in all luminal subtypes (p<0.001), while PIK3CA mutations were more frequent in Luminal A and less commonly observed in HER2-enriched tumors (p=0.001). PTEN-loss was associated with higher grade (p<0.001), higher TILs density (p=0.011) and higher proliferation rate (p=0.002), in line with its prevalence in ER/PgR-negative tumors. By contrast, PIK3CA mutations were associated with lower grade (p<0.001), marginally lower TILs density (p=0.058) and lower proliferation rate (p<0.001), in line with their prevalence in ER/PgR-positive disease. The above described characteristics of PTEN-loss were exaggerated for tumors with single PTEN-loss. PTEN-loss & PIK3CA mutations rarely coexisted in the HER2-positive subtypes, while single PIK3CA mutations were infrequent in TNBC (p<0.001). PTEN-loss/PIK3CA-mutation patterns were similar with the multi-scale IHC Approach B.
PTEN-loss and PIK3CA mutations on patient outcome. In the entire cohort of 1265 patients, 174 (13.8%) relapses and 102 (8.1%) deaths were recorded; at a median follow-up of 64.8 months (mean=62.2 months, range=2-90 months) median DFS and OS had not been reached. Patients who had breast conserving surgery, received adjuvant hormonotherapy, had lower nodal burden and tumors of lower size, lower grade, and lower proliferation rate suffered less relapses and deaths compared to the opposite conditions.
In the entire cohort and upon univariate analysis, patients with PTEN-loss fared significantly worse than patients with preserved PTEN protein expression (Figure 3, A and B) exhibiting higher risk for relapse and death (DFS: HR=1.65, 95%CI=1.22-2.23, Wald's p=0.001; OS: HR=2.12, 95%CI= 1.44-3.12, p<0.001). PIK3CA mutations were not associated with relapse and death. Single PTEN-loss was associated with significantly more relapses and deaths compared to the “normal” condition for these two molecules (no PTEN-loss, no PIK3CA mutations) and to single PIK3CA-mutations (Figure 3C and D); patients with tumors exhibiting both PTEN-loss and PIK3CA mutations had similar outcomes as those without these alterations.
In patients with HER2-positive tumors, the above statistical significance of unfavorable PTEN-loss was not retained but the overall effect of PTEN-loss was in the same direction after the 3rd year (Figure 3, E and F). Preservation of the trends for single unfavorable PTEN-loss and favorable PIK3CA mutations was noticed, but the numbers in the categories of this combined variable were partially very small for reliable comparisons.
Upon adjusting for all the significant clinicopathological variables described above, PTEN-loss and single PTEN-loss retained their unfavorable prognostic significance in the entire cohort for both DFS and OS, while single PIK3CA-mutations remained as an independent favorable prognostic factor (Figure 4). Except for the clinicopathological variables, all of which retained their independent prognostic significance, increased TILs density was also an independent favorable prognosticator in the entire cohort. In patients with HER2-positive tumors, increased TILs density was an independent favorable prognostic parameter for both DFS and OS, while PTEN-loss exhibited a non-significant trend as an unfavorable prognosticator.
All the above results with respect to PTEN-loss were obtained with the binary IHC Approach A. Similar results were also obtained in the entire cohort with the multi-scale Approach B upon log-rank testing. With respect to HER2-positive disease, IHC method discrepancy resulted in less than half patients with PTEN-loss, when assessed with Approach B. The outcome of these patients was apparently not different compared to HER2-positives without PTEN-loss. An independent unfavorable prognostic effect was yielded for PTEN-loss upon multivariate analysis; however, the corresponding group of HER2-positive tumors with PTEN-loss was too small for statistical reliability.
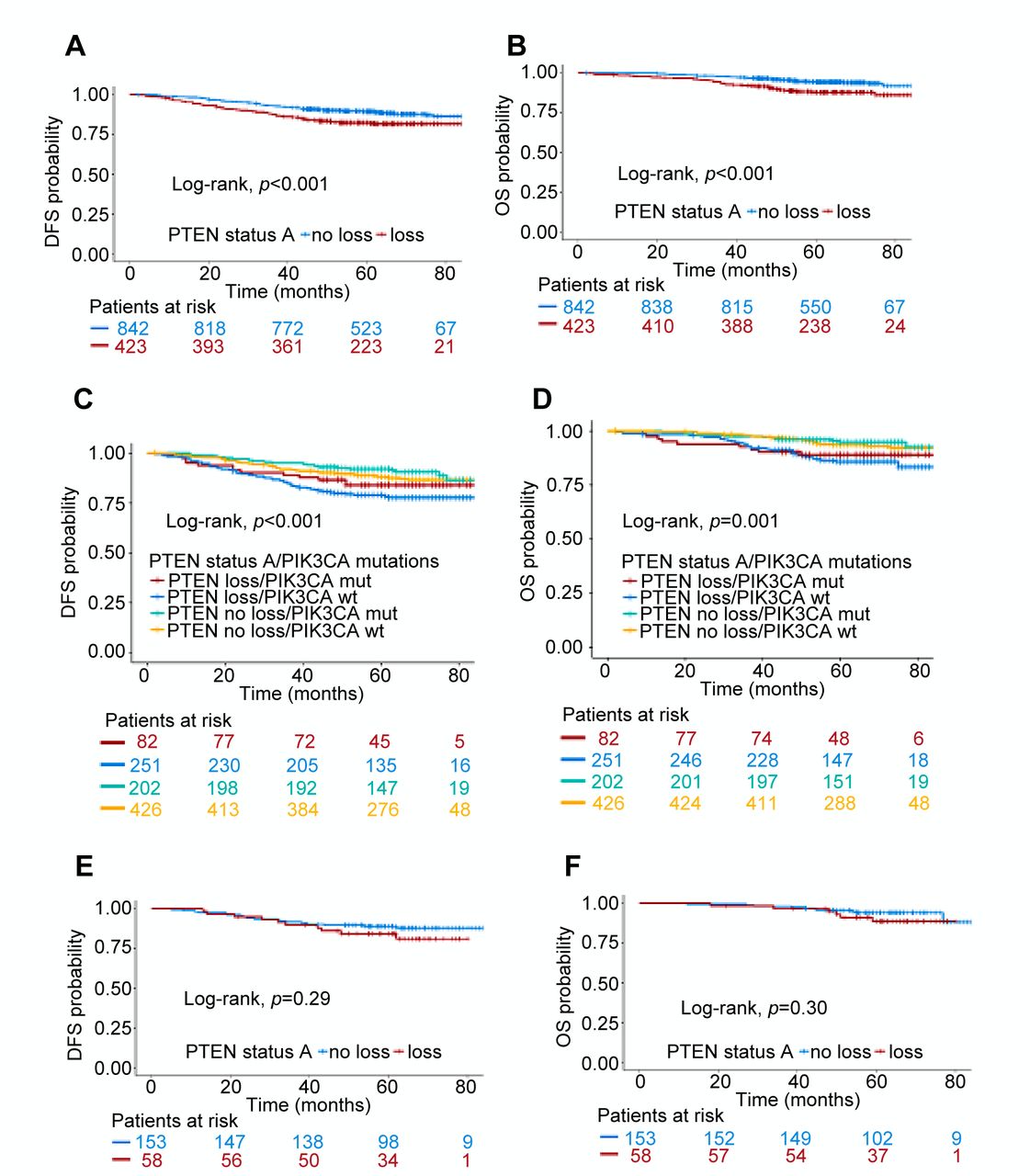
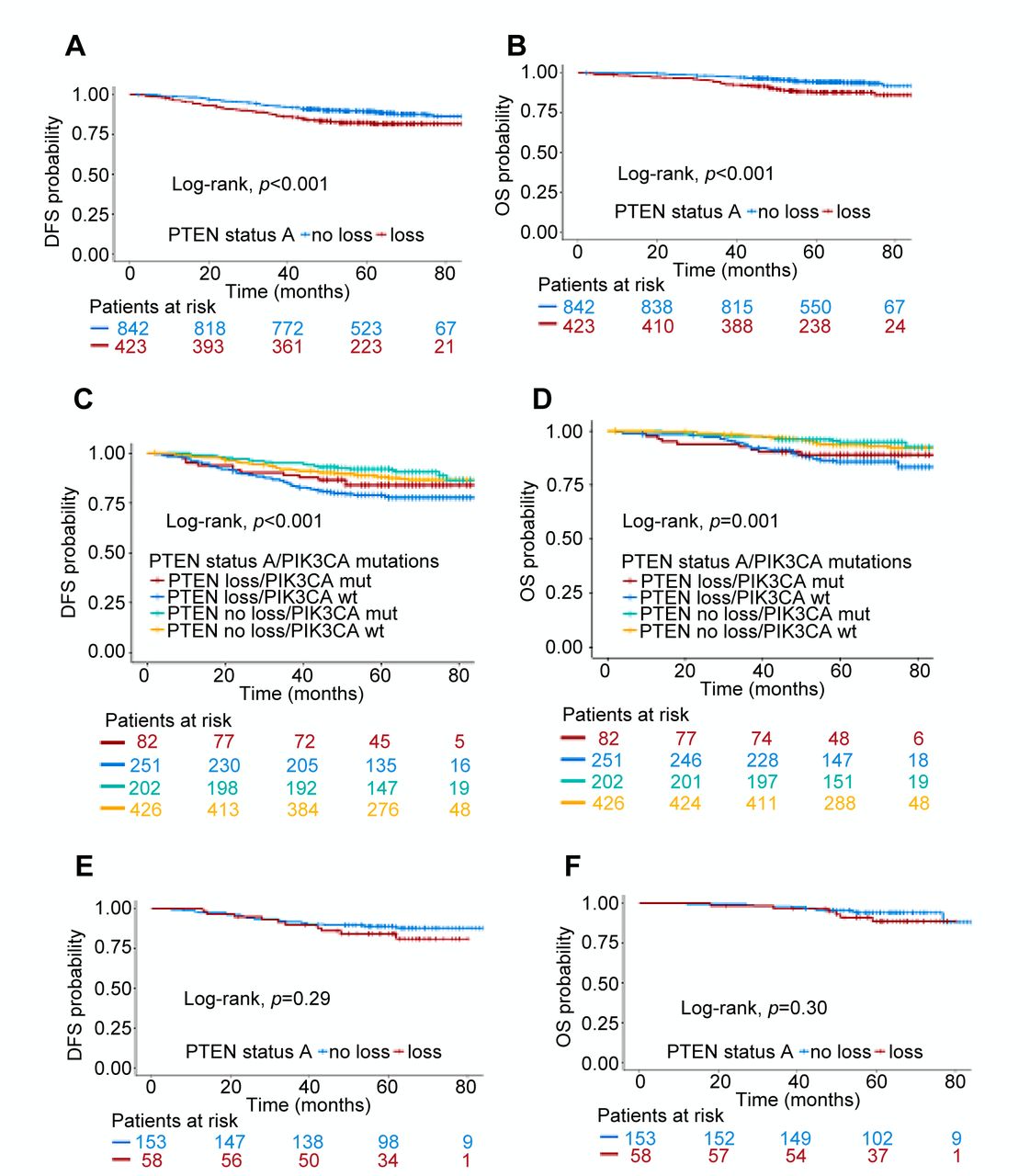
Association of PTEN-loss with patient disease-free (DFS) and overall survival (OS). A & B: PTEN status in the entire cohort. C & D: Combined PTEN/PIK3CA alterations in the entire cohort. E & F: PTEN status in HER2-positive patients. All panels: PTEN status evaluated with the binary IHC Approach A.
Discussion
Approximately 55% of early high-risk breast cancers in the present series demonstrated PTEN-loss and/or PIK3CA mutations, as generally reported (1, 19). Out of the two markers, PTEN-loss was independently associated with an aggravated outcome in patients treated with adjuvant chemotherapy, in line with a meta-analysis on the adverse impact of PTEN-loss in all stages of breast cancer (15). The novel finding here is that, when present singly, PTEN-loss and PIK3CA mutations are associated with opposite prognosis. The opposite impact of single PTEN-loss and PIK3CA mutations was fully compatible with the observed associations of these markers with clinicopathological characteristics. In comparison, in the relatively few tumors with co-altered PTEN and PIK3CA, the unfavourable effect of PTEN prevailed in the first years, indicating an inverse interaction between PTEN-loss and PIK3CA mutations. This finding is related to our previous observation in a different cohort of patients treated in the pre-trastuzumab era (16), where PIK3CA mutation types interacted with PTEN status and affected outcome in opposite directions. Further in breast cancer, TP53 mutation status may influence the prognostic effect of PIK3CA mutations (25) and of preserved PTEN (34), while the unfavourable effect of PTEN-loss may be augmented in the presence of additional alterations interfering with the activation of the PI3K pathway (35). All this argumentation suggests that we need to shift our view from single oncogenic drivers to a molecular environment that certainly interferes with- and may alter the effects of these drivers (36). PTEN and PIK3CA alterations are considered as oncogenic drivers within the same pathway but may counteract each other, e.g., in experimental models investigating sensitivity to mTOR inhibitors (37). The opposing effects of single PTEN-loss and PIK3CA mutations further support concerns that these two alterations may be inadequate as markers of PI3K activation for selecting patients to receive inhibitors of this pathway (19, 38, 39). Our finding is important to consider when designing clinical trials for testing PI3K inhibitors, where PIK3CA mutations and PTEN-loss may need to be co-evaluated.

Forest plot demonstrating the impact of PTEN status on DFS, alone and in combination with PIK3CA status in the entire cohort and in HER2-positive patients. PTEN status evaluated with the binary IHC Approach A.
PTEN-loss as a marker suffers from method and assay standardization, which has mainly prevented its inclusion in the last ASCO recommendations for markers in the adjuvant setting in breast cancer (40). Here, we applied two methodological approaches for the evaluation of PTEN IHC: one, upfront binary (loss/no-loss), similar to most previously reported studies dealing with PTEN-loss (14, 17) including our own (16, 41); the other, initially multi-scale, was based on the intensity of PTEN protein expression in the tumor stroma (11). We found that the difference between the two methods for the final evaluation of PTEN-loss is due (i) to tumors with low or very low PTEN protein expression, and (ii) to intra-tumoral PTEN heterogeneity, which is a novel finding. For the first point, low protein expression, especially when classification is based on staining intensity, is a known issue for calling a marker positive or negative with IHC. Such “grey zone” tumors that switch class from PTEN-no-loss to PTEN-loss or from PTEN-high to PTEN-low according to the method used for evaluation, as previously reported (17), constituted about 15% of all tumors in the present series. Particularly in breast cancer, given that even subtle differences in PTEN expression may be important for its biological implications (6); PTEN-loss is often used for PTEN-low although these are biologically distinct (11); genomic PTEN alterations underlying PTEN-loss or low expression are infrequent (5) or may be the result of mutational processes unrelated to PTEN itself (32); it appears doubtful that PTEN status assessed with IHC will ever be appreciated as a marker of clinical value.
Further complicating PTEN-loss as a potential marker for clinical evaluation is its heterogeneous state in primary breast tumors. We observed heterogeneous PTEN-loss in 8-13% of tumors according to the method used, although the prevalence of this condition might actually be higher since we only used TMA cores in the present study. Intra-tumoral heterogeneity mostly concerned “grey zone” tumors and may be attributed to non-genomic PTEN alterations in breast cancer (4, 5, 32). However, it may also reflect the presence of different subclones with and without genomic PTEN alterations in the same tumor, as we show here in the limited subset of tumors with PTEN mutations that were mostly represented in tumor subpopulations. Subclonal PTEN alterations in primary tumors may become overt in metastases and result in treatment failure (42). As a method, IHC may aid in assessing PTEN status heterogeneity but again, heterogeneous tumors can be classified as PTEN-loss or as no-loss with equally sound argumentation.
The incidence of PTEN-loss in the present series, 33% and 22% according to the approach used for IHC evaluation, lies within the previously described range for this alteration in breast cancer, e.g., 21% and 46% (11), 37% (43), 48% (14). With respect to breast cancer subtypes, PTEN-loss is reported as a feature of ER/PgR negative and HER2 negative disease, concerning mainly TNBC (11, 13, 32), unlike PIK3CA mutations that are characteristic for ER-positive disease (5, 24, 25, 33, 44). The presented patterns of PTEN-loss and PIK3CA mutations are in line with these reports, but we also observed a 20% incidence of PTEN-loss in HER2-enriched tumors (HER2-positive/ER-negative) compared to less than 10% in luminal-HER2 (triple positive), which is in line with the notion that luminal-HER2 is more an ER-driven than a HER2-driven disease (45). PTEN-loss is reported with variable incidence in HER2-positive disease (11, 17, 44), which may reflect issues in terminology concerning PTEN-loss vs. PTEN-low (11); methodology, concerning modes of IHC evaluation (17) as shown here as well; and, biology, since complete PTEN-loss may not be biologically relevant in a molecular environment dominated by at least one oncogenic driver, such as HER2 over-expression (32). Our results on a high incidence of PTEN “grey zone” and heterogeneous tumors in HER2-positive disease are in line with these literature data and may explain why PTEN-loss did not significantly impact the outcome of HER2-positive cancer treated in the adjuvant setting with chemotherapy and trastuzumab, as previously observed (11, 17, 44).
In conclusion, in early high-risk breast cancer, PTEN-loss is an unfavourable prognosticator, while single PTEN-loss and PIK3CA mutations may confer opposite effects on patient outcome. This finding has implications in the design of trials testing for PI3K-inhibitors. We also demonstrated that the method used for the evaluation of PTEN status with IHC and the heterogeneity of PTEN expression within the same tumor affect the classification of PTEN-loss and therefore, the statistical power of the performed analyses and the significance of this marker. These methodology issues are particularly important for the evaluation of PTEN status in HER2-positive disease exhibiting low rates of PTEN-loss, but high rates of PTEN “grey zone” and heterogeneity. Redirecting our efforts towards the search of contributors to PTEN inactivation, despite its low expression, may prove more useful for identifying intra-cellular markers of trastuzumab resistance and sensitivity to PI3K-inhibitors.
Acknowledgements
The Authors are indebted to all patients and their families for their trust and participation in the Hellenic Cooperative Oncology Group trials and for the provision of biological material for research purposes. The Authors wish to thank Eneida Jaupaj for tissue samples collection and Maria Moschoni for data coordination.
Footnotes
↵* The first two Authors contributed equally to this work.
Authors' Contributions
Study conception: GL. VK, GF; Study Design: GL, VK, IK, ET, GF; Acquisition of data: GL, EV, MB, MS, GP, EE, APB, AP, CC, HG, AK, ET, DP, FZ, GF; Analysis and interpretation: GL, VK, EV, KM, KP, EG, MB, ET, GF; Drafted the manuscript: GL, VK, IK, KM, KP, EG, Et, GE. All Authors have revised and approved the manuscript.
This article is freely accessible online.
Funding
This study was supported by a Hellenic Society for Medical Oncology (HeSMO) grant and by an internal Hellenic Cooperative Oncology Group (HeCOG) translational research grant (HE TRANS_BR). The funders played no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Conflicts of Interest
G. Lazaridis: Remuneration: Lecture Honoraria by BMS, MSD, Roche, Amgen, LEO Pharma. Consultation/Advisory role: Merck. Funding: Scholarship by HeSMO (Hellenic Society of Medical Oncology); C. Christodoulou: Consultation/Advisory role: Roche, Genesis, Pfizer, Novartis, MSD, BMS, Astra-Zeneca, Eli Lilly; H. Gogas: Funding: Novartis, Roche (Institution grant); G. Fountzilas: Remuneration: Honoraria by Astra-Zeneca. Consultation/Advisory role: Pfizer, Sanofi, Roche; The rest of the Authors declare no conflict of interest.
- Received February 11, 2019.
- Revision received March 28, 2019.
- Accepted March 29, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved




{kind=link}
{kind=link}
{kind=link}
{kind=link}